Screening of breast cancer is a complex problem. Risk scores generally perform poorly; a systematic review of the literature for the performance of the Gail model for predicting breast cancer risk found AUCs that were typically between 0.55 and 0.65 (a random classifier would have an AUC of 0.5) (Wang et al., 2018).
The next least invasive test for breast cancer screening is a clinical breast exam or self-breast exam. The sensitivity and specificity for breast exams vary widely according to age, breast density, and research setting; one study found that sensitivity can be as low as 57%, although the same study found the specificity to be 88% (Baines et al., 1989). Because a good screening test has a high sensitivity, there is a consensus that physical breast examination alone is not adequate for breast cancer screening.
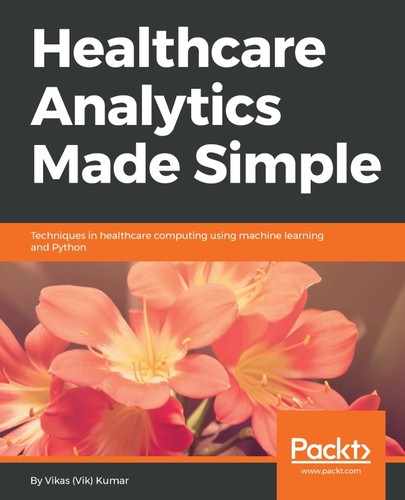
Imaging is the next least invasive screening test for breast cancer. Imaging modalities used for breast cancer screening include mammography, MRI, and ultrasound. In 2016, the US Preventive Services Task Force (USPSTF) recommended biennial mammograms (see the following diagram showing a mammogram of the breast with a whitish area diagnosed as colloid carcinoma; National Cancer Institute, 1990) for women aged 50 and older, due to the high sensitivity (77% to 95%) and high specificity (94% to 97%) of mammograms in this age group combined with their low potential for causing patient harm (US Preventive Services Task Force, 2016).
Biopsies are the most invasive options for breast cancer detection, and in fact, are used for definitive diagnosis when screening tests are positive.