
5
A Review of Innovation to Human Augmentation in Brain-Machine Interface – Potential, Limitation, and Incorporation of AI
T. Graceshalini1*, S. Rathnamala2† and M. Prabhanantha Kumar3
1Vellammal College of Engineering and Technology, Madurai, Tamilnadu, India
2Sethu Institute of Technology, Virudhunagar, Tamilnadu, India
3Vellore Institute of Technology, Vellore,Tamilnadu, India
Abstract
The beginning of Industrial Revolution in late 1700s manifested a revolving fact in the history of humans: a phase for effective and increasing human beings/ machinery interactions. In the coming decades, there were many more inventions followed, which gave rise to an increasing sense of interest and a need for imagination. Several areas of human capacity development were addressed. These are (i) neurotechnology, (ii) nootropics, (iii) genetic engineering, and (iv) brain-computer interfaces, ordered by increasing the possibility of implementation in the global economy. Brain-machine interface (BMI) utilizes existing neuroscience and engineering expertise to enable voluntary, thought-oriented control of external machines. This study underlines the increasing ability of BMI and BMI technologies to be introduced into our sector. The study also shows the limitations needed to push BMI technology out of infancy and incorporate it into artificial intelligence.
Keywords: Human augmentation, neurotechnology, brain-computer interfaces, global economy, brain-computer interfacing, artificial intelligence
5.1 Introduction
A fusion of technical capabilities enables the creation of “intelligent” brain-machine interface (BMI) [1] designs using machine learning and artificial intelligence (AI). The goal of this current technological wave is to interact in ways that foster relationship learning and adapting to new practical needs. It involves both restore-based disruptive neuronal behavior and non-invasive indicators mechanisms such as neural prosthesis electroencephalography (EEGs) [2]. Advances in BMI nanoengineering capabilities in computers, hardware, and algorithms that learn and evolve qualitatively are exploited. Finally, they are capable of understanding and adapting in (near) real-time to external environmental and physiological needs. Finally, the idea is to create a human experience for applications such as gaming, allowing the device to adapt and react in different clinical circumstances to changing events. In this comment, the ability, reasons, and technological state of the gadgets to produce them are discussed. We currently discuss a multitude of themes and difficulties in technology. Brain and Brain-computer interfaces are systems meant to connect with the central nervous system, including the brain, spinal cord, and sensory neural retina, which can be interchangeably used in this context. In addition to conducting preprogrammed neural control via an outside computer, or for brain stimulation, brain pulses are frequently acquired and clinically evaluated to restore brain activity following damage or discomfort, according to the purpose and aim of the technology. Any method, whether biochemical or through patient direction and desires, uses feedback to increase performance [3]. Furthermore, there is an increasing list of non-invasive brain interface technologies, the majority of which are funded by innovative start-ups and are not designed for therapeutic purposes. These strategies are being applied to enhance the user experience and control interfaces in sports augmented reality (AR), and virtual reality (VR). While this is an important demand, it is distinct from technology used to treat and recover patients’ health functions and quality of life [4]. Not least because it can pave the way for scientifically relevant studies. Advances in neurophysiology, computational biology, signal processing, and hardware statistical and engineering dimensions, for example, will have a major effect on the gaming, medical device, and neural prosthesis industries. The market for brain-machine engagement is projected to hit $1.46 billion by 2020, with a CAGR of 11.5 percent expected to reach $1.72 billion by 2022, with a further provision for a CAGR of 11.5 percent between 2012 and 2022. Because of the expected expansion of all of these non-invasive technologies, the game industry has almost surpassed medical applications as a market leader [5]. Despite their importance, these predictions largely represent the interaction between neural controllers and sensory experiments with robots. They are not chances that have been inserted into the craft’s present condition. BMI that can learn and evolve represents cutting-edge advances in what is possible through BMI technology integration, including nanotechnologies, artificial learning, and AI. AI can be used to create “intelligent” BMIs that can learn and adapt to evolving functional demands and needs [6].
This allows for interaction with human gamers and AR/VR [7], as well as the enhancement and creation of therapeutic applications for patients with chronic diseases. This last point cannot be overstated, since not only are the medical needs of various neurological diseases met, but it is also important to customize BMI to patients’ needs. It would also contribute to changing the technology for people’s disease evolution over time. The idea that both have one size is the primary fault of the present state-of-the-art BMI and neural prosthesis. This means that all patients can be treated correctly with a technology that operates within a particular collection or spectrum of features. Although we do not know of a system or technology which mirrors the upgraded inclusion of BMI machine learning and nanotechnology, we argued that this topic is worth exploring because of its potential and effect. All is now [8] employed in the design and functioning of BMI and neural prosthesis on its own, machine learning and nanotechnology in a series of ways that match the vision we presented here.
5.2 Technologies in Neuroscience for Recording and Influencing Brain Activity
[9] In developing new neuronal acquisition strategies and activation, cognitive processes such as vision, recollection, concentration, and preparation and execution of actions have evolved. The effects on cognitive improvement, neural interpretable control, and/or stimulation of particular target areas of the brain, but also a host of other related variables, are not the only contingent. This includes the extent to which technology needs instrumentation into the body, as well as other functional factors such as how compact and costly devices are, which affect its usefulness for human cognitive enhancement in daily life [10]. We will analyze these innovations in the following parts with their advantages and disadvantages.
5.2.1 Brain Activity Recording Technologies
5.2.1.1 A Non-Invasive Recording Methodology
[11] EEG (Electroencephalography) and near-infrared functional spectroscopy are the most widely utilized noninvasive methods for recording neural activity. EEG monitors electrical electrodes mounted on the scalp. One of the key benefits of EEG is that it has very high temporal precision, is comparatively affordable and portable to use when it comes to outdoor use for cognitive enrichment compared with other non-invasive recording techniques. However, usually, spatial resolution is limited [12]. The FMRI detects variations in blood supply (hemodynamic reaction) in the brain, monitors brain function. The spatial resolution is much better on comparing EEG, but the temporal resolution is small. Sadly, for signal acquisition fMRI requires large and costly facilities. For these purposes, it is usually unsuitable for human augmentation applications despite little effort to use it for contact. fNIRS, like fMRI, uses the hemodynamic response to assess the location and duration of brain activity. Its key advantages are its compact size, lower cost than fMRI, and lower sensitivity to electrical noise than EEG. These technologies have enhanced cognitive enhancement technology, particularly when coupled with technologies such as brain stimulation, to improve spatial work memory. FNIRS does, however, have poor space and time resolutions. MEG, which is commonly used to assess the functions of certain brain areas, locate regions impacted by anatomy as well as other diagnostic uses, is another non-invasive technology. Similar to fMRI, however, MEGs are bulky, need a magnetically shielded laboratory, and are costly [13]. For these purposes, MEG is not practicable for human increase, although some implementations are suggested based on this.
5.2.1.2 An Invasive Recording Methodology
Invasive devices use electrodes that are mounted either on the brain or the surface of the brain [8]. Therefore, recordings with a decent temporal and spatial resolution are usually less influenced by noise and distortions caused by the skull and the scalp. Implanting electrodes, however, involves brain operation to make these procedures costly and to present future ethical problems. Electrocardiograph (ECoG) [14] is an invasive technique like EEG in which neuronally produced electrode testing is performed directly on a brain, unlike EEG electrodes. EcoG screens are often just a very small region of the brain for neural activity. However, ECoG-dependent applications for cognitive human development exist. The brain microelectrode needle-shaped clusters are other invasive tools. They emit powerful but only minimal, accurate noise signals (i.e., the entire electrode measures the electrical activities of one or more neurons). For example, Gerhardt and his colleagues build invasive electrodes with ceramic foundations. Due to their extensive layout and the presence of many pads on their surface, the electrodes provide high-density, high-precision multiple recordings in deep brain areas and electrical stimulation. Invasive recording methods have the downside of only penetrating small portions of the brain, but modern developments have allowed us to look at even wider areas [15]. Due to the dangers of neurosurgery (although see [16]) and its related ethical problems, most research on non-human primates through the use of microelectrodes has been performed. Research on humans, particularly people with motor disorders and cognitive enhancement, has only been much less commonly carried out. Figure 5.1 represents the basic anatomy of the brain and its related functions.

Figure 5.1 Anatomy of the brain and its functions.
5.3 Neuroscience Technology Applications for Human Augmentation
This segment examines the key applications of human cognitive increase neuroscience technology. Many of the applications come within two general areas: Neuroergonomics and brain-computer interfaces (BCIs). Neuroergonome studies and uses this expertise to develop structures that allow people to perform more safely, more efficiently, and efficiently in daily activities and workplaces [17]. Instead, BCIs have historically focused more attention on offering ways of compensating people with serious motor impairments for lack or lost mobility, for instance enabling them to operate appliances like wheelchairs or screen cursors or to connect when the natural communication method has been badly lost. There is a substantial correlation between BCIs and neuro ergonomic systems as a broad concept of human cognitive augmentation considering any increase over the functionality currently available to a person [17, 18]. The key distinctions are the user class and program fields of concern for these users. These distinctions, however, are becoming less clear: neuroergonomics for recovery, for instance, and BCIs were used to enhance decision-making incompetent people [19, 20].
Moreover, with BCI technologies developing further, BCI spellers and pointer control systems, which are still usable for seriously challenged people, maybe “competitive” with products used currently by customers [21]. Moreover, a random control (i.e. not specifically caused by the BCI) and behavior of new BCI variations, such as passive BCIs, now fill the divide between neuroergonomics and BCIs. For these reasons, we will not attempt to distinguish neuroergonomics from BCI-related applications and will not exclude applications based on their user base size and architecture [22]. We would instead concentrate on what cognitive functions each implementation wants to enhance, as mentioned above.
5.3.1 Need for BMI
The brain-based technology interface is a growing topic, and many companies have been focused on innovating and facilitating daily chores. One of the concerns that emerge is why BMI systems are needed? BMI is a sophisticated technique, but it certainly leads to an easier existence. The reasons for focusing on this technology are as follows [23]:
- Device control may be simpler by our ideas
- It takes a little time to choose a task, whereas it is easier to run an appliance by using ideas or our brain waves technically
- Re-establish communication lines of brain and assist persons artificial limbs related to brain
5.3.1.1 Need of BMI Individuals for Re-Establishing the Control and Communication of Motor
The huge range of neurological disorders like engine neurons and backbone injuries, might cause severe motor muscular paralysis, restricting patients to artificial devices controlled by a few muscles, thereby being referred to as a ‘locking in.’ The normal channel from the brain to the limb is damaged, and BMI is used to re-establish connection alternately. BMI systems can even be used by a healthy person to operate applications in a range of user activities via the brain signal [24].
5.3.1.2 Brain-Computer Interface Noninvasive Research at Wadsworth Center
The Wadsworth Center study has explored numerous ways employed by the BMI to control a computer cursor to analyze its advantages and inconveniences, including sensory rhythm direct, which is adaptable to the potential created by motor imaging and linear regression by employing the choice of frequency-domain characteristics [25]. The other option was the cursor P300, which focuses on the sign and provides a matrix in which stimuli of varying durations may be produced. The method of Linear regression is employed for allowing those signals, like a control input, to move the cursor. The study revealed that the BMI is a methodology applied and fully user-driven; the EEG characteristics regulate speed, precision, bit rate, and usefulness of the BMI system. The sensor motor rhythms are a method that uses superior results in screen control management activities, but the P300-BCI system was lent than SMR-BMI [26].
5.3.1.3 An Interface of Berlin Brain-Computer: Machine Learning-Dependent of User-Specific Brain States Detection
The scientists at the brain-computer Berlin interface active sensory-motor rhythms, such as moving the right or the left hand and utilizing the system to determine the user’s particular brain states. When tested for their trained models, they reached a data transmission rate of over 35 bits per minute, and the total spelled output was 4.5 letters per minute (including error correction, an EEG 128-Channel, and a feedback check for unapprenticed users) [27, 28].
5.4 History of BMI
The history of BMIs is tied directly to the quest for creating new electrophysiological methods for recording the extracellular electrical activity of huge neural populations with the use of multi-electrodes [29]. Studies already mentioned in the introduction In the 1950s, a pioneer of the present BMI design was John Cunningham Lilly, then a principal investigator of the national health institutes. On or on the surface of the pial cortex, Lilly was able to implant 25–610 electrodes in adult rhesus monkeys [30] (Figure 5.2).
Besides capturing field potential (25 channels at a time), Lilly also used electronic current via these electrodes to elicit movement both in anesthetic and eave monkeys, where animals demonstrated a range of competencies and states (arm motions, sleep, etc.) [31]. He observes that there are several cortical locations, including M1 and S1, that engine responses can be called up. Lilly determined that the distinction between cortical areas was not distinct, supposed to be alone motor or sensory. Instead, he proposed to identify these sections as sensor motors. The following intermediate stage in developing the BMI idea is the advent of “EEG biofeedback” or “neuro-feedback,” particularly popular in many experimental environments in the 1960s and 1970s. The studies indicated participants about their brain activity such as auditory or visual feedback from EEG data which helped their self-regulation. In animal and human patients, David Nowlis, and Joe Kamiya [32] recorded and turned EEGs to sound. These types of neurofeedback assisted those who gained control of their EEG activities. Maurice Sterman [33] has transformed and accomplished seizure reduction using this kind of neurofeedback training EEGs for epilepsy patients in light and color. In 1963, Gray Walter [34] presented the first experiment in which humans provided brain impulses for an outside device in discussions with the Osler Society at Oxford University. It may not be fully true or verifiable Dennett’s version, as Walter did not publish the speech himself. Nevertheless, published literature shows that Walter and his colleagues implanted and utilized multiple electrodes (up to 1000) in the cortex in neurological implants for several months to measure cortical field potential. In the tests reported by Dennett, Walters recorded the potentials of motor cortex preparedness before motions, which are also categorized as ‘Bereit shafts potentials’. Pressing the button was automatic [35]. The possibility for ready led the movement around a half-second and was powerful enough to be identified by the recording equipment from Walter. Walter then managed to establish a direct connection between the motor cortex of each patient and the projector. The key was electrically unplugged from the projector and the slides were forwarded by the motor cortical readiness capabilities in this experimental situation which we now would name the brain control. The patients were surprised that even before physically initiating motion, the projector reacted to their intent. While Walter’s tests may be seen as the earliest demonstration of a possible BMI construction idea, he never published or interpreted these results in the BMI context, even though he researched artificial brain robots in his previous career in the 1950s [36, 37]. In the late 1960s, researchers at the NIH Neural Control Laboratory started experimenting with the option of using cortical neuron recording to control artificial actuators [38]. They also aimed to use direct links between brains and external equipment to restore hearing to the surviving person, paraplegic person, and blind person [39]. The study took place at specific universities and medical schools, with the cooperation of subcontractors. “We will focus on creating concepts and methods for the operation of external devices such as predictive devices, communications equipment, telecommunication operators, and perhaps even nervous system information computers.” said Karl Frank, the NIH Laboratory Chief [40]. The NIH team initially put into the primary motor cortex five microelectrodes (M1) that featured signals and then saw the action potential generated by 3–8 M1 neurons [41]. Since these neural impulses were eventually translated into the motion of an outside device, the researchers examined whether the recorded activity of tiny neural populations might anticipate wrist motions in the process. As a prediction algorithm, they used multiple linear regression. Neuronal rates were used as inputs and movie cinematic rates returned to their output. After 10 years of investigation, it demonstrated in real-time the movement of a cursor on the LED-screen by a Rhesus monkey using its nerve activity as a direct motor source with a size of 12 microelectrodes implanted in M1 at 37 mph. At the end of the ‘60s, when they used the electrical activity of individual neurons as neurofeedback’s in monkey M1, Eberhard Fetz, and his colleague researchers took place [42]. With this system, the monkeys learned how to control their neuron activity. Normally, one neuron was tested at the same time. Feedback from the audience (click for each point) or visual feedback (transferred to the rate of neuronal activity). Monkeys learned to control each M1 neuron’s activity willingly to achieve a certain firing level needed for a reward. Brindley and Craggs have employed epidural recordings of cortical field potential in the frequency range of 80 to 250 Hz in children to investigate the possibilities of developing engine neuro-prosthetic treatment that detects the unique arm and leg generating action [43]. Craggs also used mid-thoracic baboons with complete transections of the backbone as a model for human paraplegia and recorded commands from direct cortical foot images separated from the spinal cord projection region [44]. These laboratories have also researched the extraction and/or creation of neurofeedback from the motor signals of the brain, an area that focused on the provision of information to the brain, both on the peripheral and central nervous system, via electric stimulation [45–47]. This discovery resulted in early attempts to create sensory BMI’s to restore normal perceptions to those with neurological problems that produced substantial sensory deficits. Finally, this pioneering research has yielded the most remarkable results on cochlear implants (Figure 5.3).

Figure 5.2 Adult rhesus monkey experiment over BMI.
At the same time, certain progress was made in the creation of a cortical visual prosthesis spearheaded by the Brindley and Dobelle groups [48]. These researchers used electric current in surface electrode grids for the visual cortex of blind people. With this device, blind people may sense light spots, phosphenes, and distinguish basic, multifunctional visual objects. Bach-y-Rita and his colleagues began developing blind visual replacement systems in the 1960s, based on tactile stimulation of the skin on the back of the patient [49]. This approach was called tactile image projection vision replacement. The equipment used comprised 400 solenoid stimulators, which were arranged into a range of 20 by 20. The tactile stimulation was used to recreate visual pictures acquired by a video camera, using a sense of touch, on the surface of the patient’s back. After training for 10 hours, blind patients learned to distinguish items and their positioning in space and attractions, such as the entrance frame of the room.
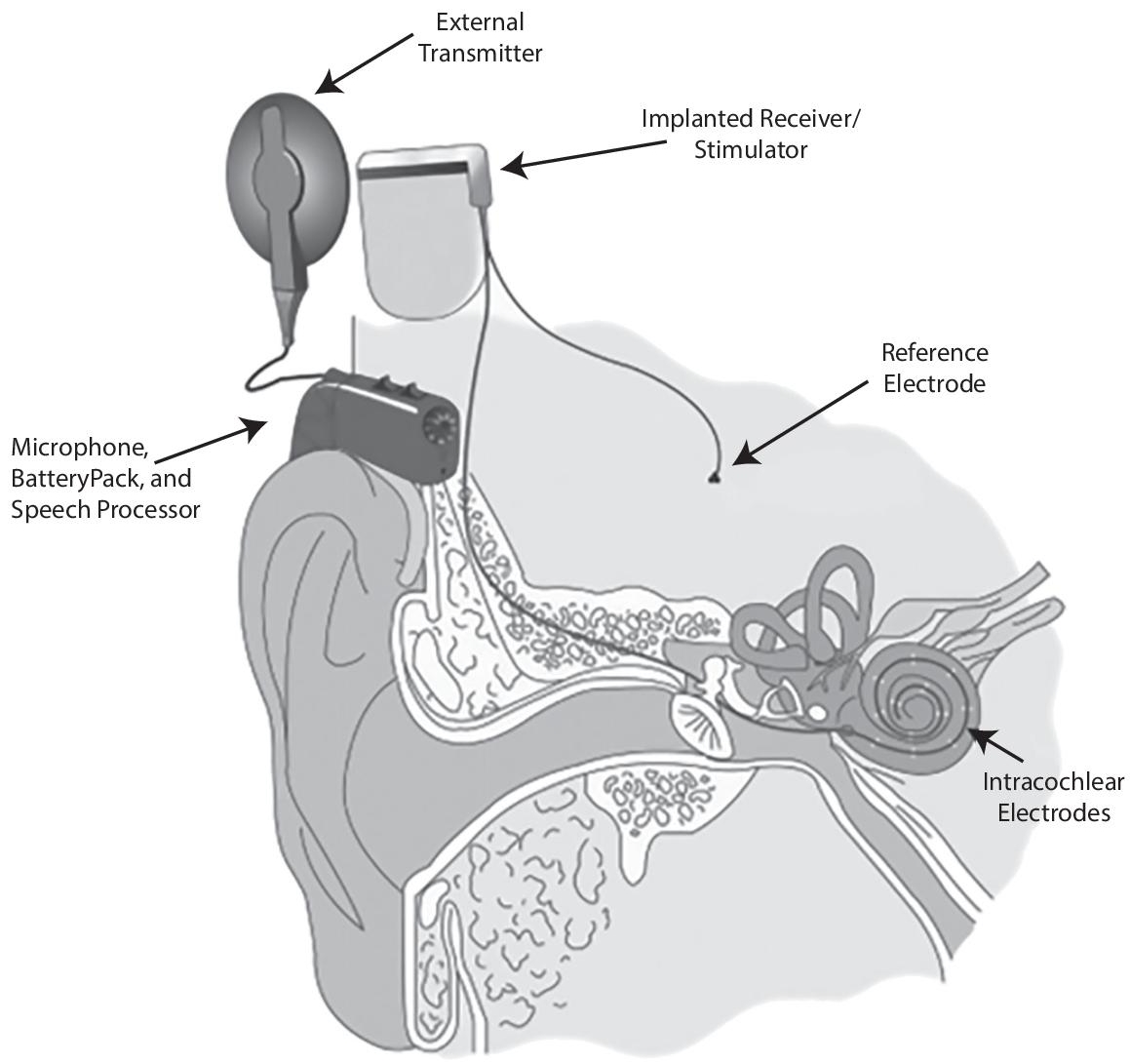
Figure 5.3 Cochlear BMI.
5.5 BMI Interpretation of Machine Learning Integration
Brain-Machine Interfaces (BMIs), to build real-time bidirectional interconnections between live brains and artificial actuators in order, integrate methodologies, ideas, and concepts originating from neurophysiology, informatics, and technology. While certain theoretical proposals and conceptual experimentation with the direct connection of brains to machines originate from the early 1960s, BMI’s research only started toward the end of the 1990s when the new neurophysiology technologies for large-scale brain activity monitoring were intimately related to these concepts [50]. BMIs have as their primary aim (1) the detection and use of operating principles and flexible qualities of the brain’s distributed and dynamic circuits and (2) the establishment of innovative treatments to restore movement and sensations for seriously damaged people. A vast array of BMI applications has arisen in the last decade, significantly broadening these basic objectives. BMI research has revealed that robots and virtual actuators exert brain control over motions that perform both upper and lower limb activities. BMIs also include ways of returning sensory inputs from external brain drives. BMI Research has led to several neurophysiologic results, including evidence of the feasibility of integrating artificial instruments through the continuous use of the monkey’s brain system. Work on BMIs has helped to discover novel techniques to retrain neurologists. This effort led to partial neurological recovery from the long-term continuous use of BMI in individuals with spinal cord injury [51]. The knowledge given by input and hardware telemetry is used to recall this algorithm. This may provide data on the current status or external data on system output settings calculated by the BMI sensors. In response to stimuli, for example, physiological measures of other algorithms outside the BMI-machine learning system, such as haptic or computer visual responses or internal parameters for current stimulus or device tracking photosystems. In the internal parameters of the algorithms, they continuously view variables such as pulse length and amplitude, stimulus rates, the use of energy in the system, the stimulation or registration density, the electrical properties (resistances, impedances) of neural tissues, and the persistent or almost permanent amounts of biochemical factors such as neurotransmission. Not one of them excludes one another, of course. Most information types and streams should be submitted in addition to the sampling resolutions, but they are likely to differ. So that the BMI produces the optimum results, which change dynamically as demands from outside contexts, machine learning algorithms can recognize subtle and no proliferating patterns and phenomena (e.g. therapeutic or operational). This includes offline architectures and algorithms, their implementation, and testing in the BMI architecture. Inappropriate parameter spaces algorithms should be able to distinguish patterns in online data. The algorithms mentioned below will decide if these data will be used separately. This step is not part of the brain interface scheme and can be accomplished using cloud algorithms if the bandwidth is necessary. However, machine-learning algorithms that classify designs inside data will undoubtedly be used in real-time to determine the board. Data transmission times and insufficient capacity would be eliminated [52]. Due to physical limitations, fewer data may also be required on the machine than can physically be preserved. To make a machine autonomous decision, the data can only be recorded for a limited time, normally as a moving window that corresponds to the processing power of the algorithm. This may also be helpful or necessary, however, the BMI system may not be necessary for offline analysis to store certain data or types of data. For example, to understand offline why machines make decisions and the health outcomes of those decisions. This step completes the closing process: the algorithms are supplied with knowledge and learned, pattern recognition, and autonomous executable decisions that in turn alter the brain-computer interface’s performance dynamically and how it communicates with the outside world [53]. In neural prostheses, a noninvasive BMI is a connector to an AR or VR system which may be the brain itself recovers the therapeutic function or device. Several research groups recognized the promise early on and are investigating how computer training can influence and combine neural stimulation with feedback. Jerbi and collaborators have created a systematic technique for recognizing motor-related signals using stochastic learning, specifically for BMI applications [54]. Most notably, the BMI training classifier does not need to be preprogrammed with comprehensive information. They were superior to other Berlin BMI IV 2008 datasets and were tested on EEG data sets with high accuracy. Their algorithms were superior. Different preprocessing methods and neural network architectures were explored in a recent analysis for EEG classification tasks. Interestingly, the data analysis in conjunction with a preprocessing phase studying the electrode system’s spectral energy conservation characteristics has been deemed appropriate in a reasonably easy networking architecture. They were in linear regression with a single convolution sheet, relationship layer, and single classifier [55]. They were able to co-adapt data training through their approach to achieve online classification. Another research has a connected methodology. The ability of the computer to learn to modulate in real-time and almost real-time the result of physiological and other internal device inputs such as the feedback of other internal processing algorithms may be one of BMI’s main advantages. Most BMIs have a decoder that decodes and makes sense of neural signals for executable or actionable output. This usually requires intensive supervised training to refine the representation of neural signals that are captured until the decoder can equate detected signals correctly with expected outputs and commands. This teaching has historically involved supervised guidance from a human on the loop. This usually involves a technician or clinician who also receives the patient’s feedback. Eventual training and modifications are rarely carried out daily and require time. In addition, neural signals that map outputs are limited to the training data which is exposed to the system during training. This significantly reduces the capacity of the BMI to respond in reality to variable particular conditions. Their versatility will then be drastically reduced to patients when complications occur. Early work was based on external sensor references input to calculate an error between the device output and the intended controlled objective. Visual and auditory signs were used. Although these methods are however strictly restricted since they involve the continued feedback of an arbitrary reference goal to change the mapping to BMI output. More recently, some of these inconveniences have been solved by the adjustment of output metrics of unattended learning approaches such as Bavarian mathematical methods and improved learning that are not externally referenced. But in most instances, they require substantial periods of preparation. Latest studies can specifically investigate and adapt endogenous neuronal signals in iterative closed feedback loops using the BMI as a training source. Chavariagga and colleagues are, for example, exploring a technique called act-critical strengthening learning that doesn’t require a supervised error signal [56].
In general, machine learning is still under consideration in the area of BMI and neural prostheses in particular. One challenge is the absence of the right solution to the constraints set by the BMI by main modern approaches, such as deep learning, which have had great success in other applications. Panuccio et al. (2018) also published an excellent report in a recent article which outlines the current state and challenges of neural engineering, aiming to restore the neural function, including a range of related criteria outlined in this report, which will need to address new algorithms and machine learning to construct an adaptive IMO. The probability of creating BMIs which can react to the space and time conditions needed to achieve realistic results is a significant factor, since such machine learning techniques make other approaches impossible. The optimal strength of the stimuli required for a goal response in neurons is a complex factor for neural stimulation and may not be the highest stimulation density possible for the system [57]. The density of stimuli can be responded in a complicated manner, which depends also on fundamental physiology and pathology. In certain cases, it is impossible to understand the right relaxing density. In addition, the optimum density of stimuli can differ from one person to another and under a common illness and, with the transition in physiology and the adaptation of the body to modified conditions, the disease can change considerably in a particular patient. This may be due to age or exogenous factors such as the patient’s response to other medications, diet, and psychiatric disorders. Another factor to remember is hardware and other algorithms that use known or calculated neural knowledge to communicate with the brain, which has various scaling requirements. It depends on the external problem and how neural data are used. The technical capacities and limitations of external data requiring technology are represented. The sample can lead to a deceptive or false AR/VR experience or a patient without a disability cannot communicate accurately or in a timely. The results are also available. Excess sampling will take time and resources for computation. The empirically defined precision of a computer model of how the theory is evaluated and understood may be impacted by data scaling problems in a testing setting. Treatment or other therapeutic choices may have a clinical effect. The change in the time and space scaling parameters needed by exogenous BMI considers situational issues, which cannot yet be considered substantially by the current state of the art. Integrating computer training and AI with the nanotechnology BMI enables you to consider, develop and respond to environmentally challenging questions like complex scaling criteria to address these challenges technically [58]. (For example: see Figure 5.4 Brain-machine interface schematics).
The extracellular activity of several hundred neurons in several cortical zones involving motor control of arm and moving is measured using intracranial recordings. A set of decoders that pull system parameters from the brain signal process the combined action of cortical neuronal ensembles in real-time. The decoder outputs are utilized to control the robot arm motions which enable human patients to carry out arm movements [59].

Figure 5.4 Brain-machine interface schematics.
The interface phases of the brain-computer system include:
- Brain measurement/BMI recorder
- Preprocessing
- Feature extraction
- Implementation and classification Machine Learning
- Signal control translation
5.6 Beyond Current Existing Methodologies: Nanomachine Learning BMI Supported
The study on nanotechnology designed to communicate and interact with the brain and central nervous system, in general, has increased in the last few years. Recently, a substantial attempt was made to record and induce high densities in the brain using nanoscale neurotechnology. The brain initiative and the Human brain project have had a major impact on federal science efforts in both the United States and the European Union. We are not here to examine this extensive literature, but rather to guide the reader to references and publications in general. Machine learning, BMI nano-engineered, and neuro-prosthesis have not yet been combined. Machine learning is becoming particularly important in other areas of molecular science and nanotechnology (for example, see the review by [60]. Albrecht et al., for example, published a tutorial on using near-transparent networks to analyze or derive molecular data from DNA sequence studies demonstrated in previous years how to improve Si-Si and Si-Ge thermal interfacial conduction using an atomic version of the mechanism and Green’s function optimization. In a library of over 60,000 candidates, their approach was able to define optimal structures. Also, existing techniques were able to create an extensive research framework built and optimized by deep learning on a 3 D-pressed Diffractive Deep Neural Network in another remarkable recent study (D2NN). Their classification and other imaging operations were possible without using or using any energy in their structures other than input light. Computer training capability (i.e. model identification and interpretation) is the capacity of BMI and neural prosthesis to consult and improve device output and operating efficiency through the use of extremely detailed physical and chemical data from sensors. However, as previously said, it is critical to recognize that the most recent computer and AI algorithms are insufficient for these requirements. Many people who can detect and use nanotechnological BMI devices can deliberately create machine learning algorithms. Current machine-learning methods, especially deep artificial neural networks (ANNs), are extremely effective. What is perhaps more disturbing is that these types of the mathematical downgrade are the foundational principles that lead to ANN’s current state-of-the-art and performance. However, theoretical and practical constraints remain, just as they do in every other framework. As a result, the data on which they function must be able to satisfy these constraints. Current algorithms, in particular, rely on exposure to large data sets to learn properly(a form of model bias). Only existing data will contain correlations and trends (model bias again). There is always a risk that a small training set would generalize (model overfitting). In these circumstances, they show nearly full strength and the potential to adapt beyond their training sets. New information cannot be learned further (model saturation). And these reasons are why these approaches are not available (data sparseness problem). Finally, they take vast computer resources and an item of enormous energy expenditure to classify learning patterns properly. These approaches are constrained by several key problems inherent in mathematical learning engineering. However, even with that drawback and the entire buzz surrounding machines and AI at the moment, the achievements of these methods are difficult not to be impressed. If data and resources are adequate to fulfill the task of the algorithms, these proceedings will be remarkably effective, with efforts at replacing new methods likely unworkable (and even unnecessary) for the near future at least. Machine learning is suited to the present state of the art of the BMI in some ways. BMI may possess a large number of data and physiological signals, relaxation parameters, and functional densities which are sufficiently well understood to determine for extremes, at least, are operational conditions. Thus, the current machine can properly learn algorithms for decision-making to adjust the BMI to its targets, based on proven and practical physiological ranges of activity. Indeed, in a monogeneric brain-computer interface, the degree of controlling synthesis over the material or the device and space and time relaxation resolutions and the recording density can be designed. Nanogenerated BMI will deliver the output and a lot of experience, combined with the level of nanoscale Functional Control Engineering, which is particularly appropriate for using state-of-the-art machine learning and AI for smart, embedded BMIs. But it’s important to ask, whether BMIs can provide a certain amount of functionality and incorporation in machinery and AI architectures that are programmed to learn differently from existing algorithms. Machines that model complex neurobiological properties mathematically and abstractly. Specifically, empirical (i.e., data-driven) statistics perform best on problems where distortion, sparsity, and saturation do not (or cannot) restrain learning. However, outside of these boundaries, the mammalian brain is excellently understood [61]. The capacity of the brain to adjust and extrapolate beyond the outcome and its unbelievable physical and computing capability is particularly crucial. These characteristics go beyond existing computer training levels but they may be critical for the development of BMI in the brain. The human brain varies greatly from how modern neural artificial networks, deep learning, and algorithm “read” methods result from patterns. The brain much of the time is learned through analogy and a rundown. It adapts robustly to various circumstances and environments that it could not have met with an unbelievable degree of plasticity. Brain stability, adaptability, and strength of computing are higher than any existing computer. An extremes example of the extraordinary robustness of the human brain and its adaptability is a rare pediatric chronic inflammatory neurological disease, known as Rasmussen’s encephalitis, that usually affects one hemisphere. It normally has seizures that cause muscle coordination, speech loss, hemiparesis, encephalitis, and cognitive dysfunction and are very frequent. The bulk of cases are medical refractory (stop reacting). Hemispherectomy is both the first and only efficient cure for epilepsy. Part or whole of the cerebral hemisphere is separated from the unintended hemisphere by surgery. The corpus callosum is the “ribbon thread,” which divides the two ends of the brain. However, the other patients’ brains will take over the roles of the cerebral tissue excised to different degrees. In certain cases, the patients will almost naturally function psychologically and cognitively, with the volume of brain removal into consideration. (You can also compare what would happen when you uninstall any transistors or circuits on a device.) With about 20W electricity, the brain can do anything for computing efficiency and energy efficiency - insufficient for powering a dim light bulb, the “wetware” is around 3lbs, equivalent to a 2liter soda bottle. Finally, although the computational characteristics and learning ability are available, that means that we don’t have to reverse brain engineer to the point where we model or simulate a portion of how biology executes internal brain algorithms. One solution is to abstract biological knowledge and document the main algorithms, namely the legislation behind the BMI property or scheme. The result is that mathematical models are separate from fundamental bio details, but they catch realistic features to an algorithmic imitation. Of necessity, it can be more science than art if this line of abstraction is drawn.
5.7 Challenges and Open Issues
In this last part, we will present briefly some of the problems and challenges in implementing the vision above. We do not detail this text, but let the parties consult and discuss it further. First, the majority of recent attempts in developing neurotechnologies for the tracking or relaxation of high density have concentrated on the mechanics, chemistry, and engineering of key nanotechnology. This can be understood because the basic technology required to allow for activation or recording at the actual brain interface must arrive first. The data and knowledge supplied by these technologies must precede all methods or technologies for changing or using them. To ensure reliable recording or relaxation, above and above the real interface, mechanical and operating stability and long-term system durability are crucial. For instance, as the electrodes turn, or exaggerated reactive gliosis exists, they will seriously affect the efficiency and precision of the machines, making any machine learning algorithms monitoring or adaptation meaningless. These represent fundamental problems in engineering that have drawn considerable work. And though much has been achieved, very active areas of study are still available.
In addition to these familiar problems concerning the manufacturing and functionality of BMI products, there are relatively less focused, transparent problems. Questions on how to view and use data from these machines, which are of interest in any debate on incorporating machine education into the system as a whole, are of special importance. The density to record or boost can be so high on a nanoscale that the telemetry dilemma about how all these signals are to be detected is a problem. In other words, how do you monitor where signals originate and where (when records are made) (in the case of stimulation). The standard microscale method of the person ‘read out’ is physically impossible for high-density recordings, for instance, several thousand signals. Many nanotechnologies are designed into such drastic densities as standalone nano-scale instruments, which then can be used in large quantities. But, while each system can truly track local signals, how is the information collected globally over the entire sensor community, and how is this data meaningful? This issue is crucial in the case of applications requiring spatial “corticotopic” detail. We have no definitive response yet, but we cannot overestimate the impact of the issue. Whatever the answers, a mixture of nanotechnology, algorithms, and methods of data analysis are almost definitely needed. How do you selectively focus nanoscale electrodes on and on according to the specified programmed protocols, in regulated and organized spatial and temporal combinations, to create the most effective clinically significant stimulation paradigms, i.e. turning on and off. This will probably range from one patient to the next and develop in the same patient over time. As discussed above. The learning and adaptation processes used in the BMI and neural prosthesis could be at the center of the learning process to handle certain improvements. The architecture of BMI systems should comply with the installation and incorporation of machining, which is designed to operate within the overall framework from a material and engineering perspective.
Other critical aspects are wider topics that go beyond simply nanoengineered, specific, and important BMI integration with AI. For example, the neurophysiology, neural code, and purpose of neural signals are not well understood in processing information. This makes it difficult or impossible to create practical BMI learning algorithms. This makes it difficult. While neural stimulation or interface recording technologies have been mastered and efficient learning of machinery to monitor closed-loop feedback can still be developed, what we will optimize is not clear. We simply don’t understand how well the brain functions. It is the brain that adapts to engineered technology and not the opposite to modern technology for a neural prosthesis. Other open topics show open innovation challenges beyond and beyond neuroscience. How can machine learning and AI performance be extended to the device itself in terms of limited form factors and local computing capability? If access to vital computing services in the cloud is required, appropriate bandwidth access should be ensured, especially in clinically sensitive circumstances.
5.8 Conclusion
Finally, the ethical problems posed by the implementation and application of these innovations must be recognized and considered. The ethical implications of neurotechnologies and AI on their own are significant. And at least one recent commentary simultaneously addressed ethical issues in psychiatry, neurotechnology, and AI. The authors defined four concepts to be followed and respected by those technologies: anonymity, identification, agency, and equity. There must be a continuous and changing dialogue that follows technological change. The possible threats to be ignored or deferred are too high. The integration of the brain network and the brain programming interfaces of machine learning and AI provides the possibility of important neurotechnological developments. BMIs that can learn and respond to environmental and situational pressures of external demands provide enormous opportunities to dramatically transform patients’ care and quality of life. It also provides possibilities for non-invasive human-machine encounters and collaborations that are present only within the field of science fiction.
We might imagine an age of customized human journeys, impacting both clinical and non-clinical applications. As for all advancement that changes in disruption and paradigm, there are, of course, many technological problems to address, many of which are not straightforward and are serious ethical issues to consider and navigate with consideration. However, it cannot be avoided the opportunities, how we collaborate, use technology and machinery, and the evolving effect on the quality of life and well-being of the most beneficial patients. We argued that the use of modern neural Algorithms and modern machinery architectures should be taken into consideration in modeling cognitive science and neurosciences processes in machine learning and in the AI algorithms necessary to reach the interface of “smart” nano-engineered brain machines. For this reason, we have not argued for the need for general artificial intelligence (AGI) and are by no means obvious. The use of sophisticated algorithms is likely to be advanced applications such as smart adaptive BMI based on experimental evidence on current mathematical models and hypotheses. These independent algorithms are however not AGI from a context (although they could conceivably contribute to it). Substantial analyses, pattern analysis, education, and decision-making may take place in these algorithms, but only in the context and embodiment of neurotechnology. The concept of a self-aware machine or a conscious computer should not be confused with those technical considerations currently needed in this paper, namely, the subject. This is a fundamental distinction, as the regulatory questions and the continuing AGI discussions are very different from neurotechnology’s societal and ethical concerns.
References
- 1. Galiautdinov, R. and Mkrttchian, V., Brain Machine Interface for Avatar Control and Estimation for Educational Purposes Based on Neural AI Plugs: Theoretical and Methodological Aspects, in: Avatar-Based Control, Estimation, Communications, and Development of Neuron Multi-Functional Technology Platforms, pp. 294–316, IGI Global, 2020.
- 2. Jebari, K.J.N., Brain machine interface and human enhancement–An ethical review. 6, 3, 617–625, Springer, New York, USA, 2013.
- 3. Galiautdinov, R.J., II, Brain machine interface: The accurate interpretation of neurotransmitter signals targeting muscles. International Journal of Applied Research in Bioinformatics (IJARB), 10, 1, 26–36, IGI Global, Pennsylvania, USA, 2020.
- 4. Silva, G.A.J.F., II, A new frontier: The convergence of nanotechnology, brain machine interfaces, and artificial intelligence. Front. Neurosci., 12, 843, 2018.
- 5. Hortal, E., Iáñez, E., Úbeda, A., Perez-Vidal, C., Azorin, J.M.J.R., Systems, A., Combining a brain–machine interface and an electrooculography interface to perform pick and place tasks with a robotic arm. Rob. Auton. Syst., 72, 181–188, 2015.
- 6. Chen, X., Chen, J., Cheng, G., Gong, T.J.P.O., Topics and trends in artificial intelligence assisted human brain research. PLoS ONE, 15, 4, e0231192, 2020.
- 7. Jones, C., Novitzky, M., Korpela, C., AR/VR Tutorial System for Human-Robot Teaming, in: 2021 IEEE 11th Annual Computing and Communication Workshop and Conference (CCWC), pp. 0878–0882, IEEE, New York, USA, 2021.
- 8. Musk, E. J. J. O. M., II, An integrated brain-machine interface platform with thousands of channels. 21, 10, e16194, 2019.
- 9. Chen, R., Canales, A., Anikeeva, P. J. N. R. M., Neural recording and modulation technologies. 2, 2, 1–16, 2017.
- 10. Liu, D. et al., Interactive brain activity: Review and progress on EEG-based hyperscanning in social interactions. bioRxiv, 9, 1862, 4, 545–564, 2018.
- 11. Formento, E., Botros, P., Carmena, J.J.B., A non-invasive brain-machine interface via independent control of individual motor units, 2021.
- 12. Ito, H., Fujiki, S., Mori, Y., Kansaku, K.J.N.R., Self-reorganization of neuronal activation patterns in the cortex under brain-machine interface and neural operant conditioning. 156, 279–292, 2020.
- 13. Prasad, G. J. L. M. A. H. O. R., II and Systems, B., Brain-machine interfaces. 461–470, 2018.
- 14. Benabid, A.L. et al., An exoskeleton controlled by an epidural wireless brain– machine interface in a tetraplegic patient: A proof-of-concept demonstration. 18, 12, 1112–1122, 2019.
- 15. Niketeghad, S. and Pouratian, N.J.N., Brain machine interfaces for vision restoration: The current state of cortical visual prosthetics. 16, 1, 134–143, 2019.
- 16. Waldert, S.J.F., II, Invasive vs. non-invasive neuronal signals for brain-machine interfaces: Will one prevail? 10, 295, 2016.
- 17. Liao, L.-D. et al., Biosensor technologies for augmented brain–computer interfaces in the next decades. 100, 1553–1566, 2012.
- 18. Farah, M.J. and Wolpe, P. R. J. T. H. C. R., Monitoring and manipulating brain function: New neuroscience technologies and their ethical implications. 34, 3, 35–45, 2004.
- 19. Li, Z., Ruan, M., Fang, Y.J.N.B., Major depressive disorder: Advances in neuroscience research and translational applications. 1–18, 2021.
- 20. Yeung, A.W.K. et al., Virtual and augmented reality applications in medicine: analysis of the scientific literature. 23, 2, e25499, 2021.
- 21. Xu, W., Dainoff, M.J., Ge, L., Gao, Z. J. A. P. A., From human-computer interaction to human-ai interaction: New challenges and opportunities for enabling human-centered AI, 2021.
- 22. Rao, R.P., Brain-computer interfacing: An introduction, Cambridge University Press, Cambridge, England, 2013.
- 23. Kapoor, N., Furler, J., Paul, T.V., Thomas, N., Oldenburg, B. J. J. B. S., The BMI-adiposity conundrum in South Asian populations: Need for further research. 51, 4, 619–621, 2019.
- 24. Chaudhary, U., Mrachacz-Kersting, N., Birbaumer, N. J. T. J. O.P., Neuropsychological and neurophysiological aspects of brain-computer-interface (BCI) control in paralysis. 599, 9, 2351–2359, 2021.
- 25. Alonso-Valerdi, L.M. and González-Garrido, A. A. J. D. C., A. Computational neuroscience: Principles, and L. applications, IntechOpen, in: Characterizing Motor System to Improve Training Protocols Used in Brain-Machine Interfaces Based on Motor Imagery, pp. 57–76, 2018.
- 26. Leuthardt, E.C., Moran, D.W., Mullen, T.R.J.F., II, Defining surgical terminology and risk for brain computer interface technologies. 15, 172, 2021.
- 27. Abiri, R., Borhani, S., Sellers, E.W., Jiang, Y., Zhao, X. J. J. O. N. E., A comprehensive review of EEG-based brain–computer interface paradigms. 16, 1, 011001, 2019.
- 28. Lebedev, M.A., Opris, I., Casanova, M.F., Augmentation of brain function: Facts, fiction and controversy. Front. Syst. Neurosci., 12, 45, 2018.
- 29. McMullen, D.P. et al., Demonstration of a semi-autonomous hybrid brain– machine interface using human intracranial EEG, eye tracking, and computer vision to control a robotic upper limb prosthetic. 22, 4, 784–796, 2013.
- 30. Lebedev, M.A. and Nicolelis, M. A. J. P. R., Brain-machine interfaces: From basic science to neuroprostheses and neurorehabilitation. 97, 2, 767–837, 2017.
- 31. Ifft, P.J., Shokur, S., Li, Z., Lebedev, M.A., Nicolelis, M. A. J. S. T. M., A brain-machine interface enables bimanual arm movements in monkeys. 5, 210, 210ra154–210ra154, 2013.
- 32. Nowlis, D.P. and Kamiya, J.J.P., The control of electroencephalographic alpha rhythms through auditory feedback and the associated mental activity. 6, 4, 476–484, 1970.
- 33. Lucido, M.J., Effects of neurofeedback on neuropsychological functioning in an adult with autism, Walden University, Minneapolis, Minnesota, USA, 2012.
- 34. Soekadar, S.R. and Birbaumer, N. J. C. P. N. D., Clinical brain-machine interfaces. 83, 347, 172–179, 2014. https://www.sciencedirect.com/journal/neurobiology-of-disease/vol/83/suppl/C
- 35. Lorentz, H., Mach, E., Poe, E. A. J. T. B. F., II, An unmistakable difference exists between spatial and temporal concepts. 241, 2019.
- 36. Walter, W. G. J. S. A., An imitation of life. 182, 5, 42–45, 1950.
- 37. Hurst, F., Imitation of life, Duke University Press, North Carolina, USA, 2004.
- 38. Seo, D., Carmena, J.M., Rabaey, J.M., Maharbiz, M.M., Alon, E. J. J. O. N. M., Model validation of untethered, ultrasonic neural dust motes for cortical recording. 244, 114–122, 2015.
- 39. Schmidt, E.M., Cortical control of robotic devices and neuromuscular stimulators, in: Neurobionics, pp. 289–295, Elsevier, Netherlands, 1993.
- 40. Frank, K. J. A. O. O., LXII Some approaches to the technical problem of chronic excitation of peripheral nerve. Rhinol. Laryngol., 77, 4, 761–771, 1968.
- 41. Humphrey, D.R., Schmidt, E., Thompson, W.J.S., Predicting measures of motor performance from multiple cortical spike trains. 170, 3959, 758–762, 1970.
- 42. Sharif, S. and Ali, S. M. J. W. N., I Felt the Ball”–The Future of Spine Injury Recovery. 140, 602–613, 2020.
- 43. Grahn, P.J., Strategies to advance intraspinal microstimulation toward therapeutic application for restoring function following spinal cord injury. College of Medicine-Mayo Clinic, 2015.
- 44. Urbin, M., Royston, D.A., Weber, D.J., Boninger, M.L., Collinger, J. L. J. N. O. D., What is the functional relevance of reorganization in primary motor cortex after spinal cord injury? 121, 286–295, 2019.
- 45. Brindley, G. and Craggs, M. J. T. J. O. P., The electrical activity in the motor cortex that accompanies voluntary movement. 223, 1, 28P–29P, 1972.
- 46. Brindley, G. and Lewin, W. J. T. J. O. P., The visual sensations produced by electrical stimulation of the medial occipital cortex. 194, 2, 54–5P, 1968.
- 47. Libet, B., Alberts, W.W., Wright, E., Delattre, L., Levin, G., Feinstein, B., Production of threshold levels of conscious sensation by electrical stimulation of human somatosensory cortex, in: Neurophysiology of Consciousness, pp. 1–34, Springer, USA, 1993.
- 48. Dhanaraj, R.K., Krishnasamy, L. et al., Black-hole attack mitigation in medical sensor networks using the enhanced gravitational search algorithm. Int. J. Uncertain. Fuzz. Knowl.-Based Syst. 1968, 196, 2, 479–493.
- 49. Sharif, S. and Ali, S.M., Spine health special section. World Neurosurg., 140, 602–613, 2020.
- 50. Zhang, S. et al., Pain control by co-adaptive learning in a brain-machine interface. Curr. Biol., 30, 20, 3935–3944, 2020.
- 51. Myszczynska, M.A. et al., Applications of machine learning to diagnosis and treatment of neurodegenerative diseases. Nat. Rev. Neurol., 16, 8, 440–456, 2020.
- 52. Samek, W., Montavon, G., Lapuschkin, S., Anders, C.J., Müller, K.-R., Toward interpretable machine learning: Transparent deep neural networks and beyond, 2020. arXiv preprint arXiv:2003.07631.
- 53. Trajkovic, L., Brain-machine interface systems. IEEE Syst. Man Cybern. Mag., 6, 3, 4–8, 2020.
- 54. Jerbi, K. et al., Inferring hand movement kinematics from MEG, EEG and intracranial EEG: From brain-machine interfaces to motor rehabilitation. IRBM, 32, 1, 8–18, 2011.
- 55. Dhanaraj, R.K., Krishnasamy, L., Geman, O., Izdrui, D.R., Black hole and sink hole attack detection in wireless body area networks. Comput. Mater. Continua, 68, 2, 1949–1965, 2021.
- 56. Chavarriaga, R., Sobolewski, A., Millán, J.D.R., Errare machinale est: The use of error-related potentials in brain-machine interfaces. Front. Neurosci., 8, 208, 2014.
- 57. Shepherd, G.M., Corticostriatal connectivity and its role in disease. Nat. Rev. Neurosci., 14, 4, 278–291, 2013.
- 58. Chaudhary, P. and Agrawal, R., Brain Computer Interface: A new pathway to human brain, in: Cognitive computing in human cognition, pp. 99–125, Springer, USA, 2020.
- 59. Dhiviya, S., Malathy, S., Kumar, D.R., Internet of Things (IoT) elements, trends and applications. J. Comput. Theor. Nanosci., 15, 5, 1639–1643, 2018.
- 60. Wiecha, P.R., Arbouet, A., Girard, C., Muskens, O.L., Deep learning in nano-photonics: Inverse design and beyond. Photon. Res., 9, 5, B182–B200, 2021.
- 61. Angehrn, Z. et al., Artificial intelligence and machine learning applied at the point of care. Front. Pharmacol., 11, 10–15, 2020.
Notes
- *Corresponding author: [email protected]
- †Corresponding author: [email protected]