
6
The Potential of Artificial Intelligence in the Healthcare System
Meena Gupta* and Ruchika Kalra
Amity Institute of Physiotherapy, Amity University, Noida, Uttar Pradesh, India
Abstract
AI is a cross-disciplinary field of research that attempts to understand, model and replicate intelligence and cognitive processes by invoking computational, mathematical, logical, mechanical and biological principles and devices. There are various types which comes under AI, as machine learning, natural language processing, artificial neural networks, robots, expert systems and fuzzy logics. The concept behind the artificial intelligence is that to act as the copy of human, thinking, skills, language processing, and other features. AI has the potential to be used in planning and resource allocation in health and social care services. AI has the potential analyse clinical data, research publications, and professional guidelines to aid the diagnosis of disease and could also help to inform decisions about treatment. The sensor technology works as the human machine interaction with devices such as wearable and non-wearable devices which woks separately and have the best transmission with the presence of sensor nodes with this technology there is no use for the repeater and the feedback outcome comes best with the help of technology in the devices like thermal mechanism where the heat is the mediator turning mechanical to electrical energy for wearable device and in case of non-wearable device such as pacemaker in heart will initiate for the electrical energy to stimulate heart pumping. The artificial intelligence not only works privately but also in community and public healthcare which consist of experimental trials outcomes, research, private documentation which needs to be secured hence there are alarming devices named as intrusion devices which also work with sensor networking and Xerox of human immune system so as to save the data so as the T and B cells does. Utility of AI in medicine, surgery, and rehabilitation is specific with every application in the artificial intelligence. Such clinically relevant set of apps are a good example of evidence based clinical answers and skills that can be accessed as and when we need them. AI integrated mobile applications, and wearable fitness trackers, the physiotherapist can track the vitals, physical activity, exercise sessions and other parameters, without the patient having to come into the clinical setting. The future changes and requirement for AI will be increased with increased precision in all aspects which is present as in medicine, pathology, rehabilitation, but future will be facing challenges inclusive of updates in AI should follow the clinical practice as followed by the medical professionals.
Keywords: Artificial intelligence, healthcare, mobile applications, natural language processing, machine learning
6.1 Introduction
Artificial intelligence is defined as the research field of turning and replicating the intelligence and cognitive process by artificial means by computer means such as mathematical, logical, cognitive principles as shown in Figure 6.1. The artificial intelligence is cumulative form of synthesizing and analyzing the agents of computer presenting intellectual behavior [1, 2].
The artificial intelligence is upgraded and in process in the field of healthcare with various systems such as machine learning, natural learning process, expert systems, robotics, fuzzy logics which together have stepped in various diagnostics, healthcare data, clinical treatment, modeling, decision making and other healthcare services which have enhanced the accuracy and precision [3−6]. According to a literature the artificial intelligence is termed as intelligent agent which is composed of a system inclusive of actuators, sensors, agents and environment and are interlinked and terming as perception cycle of artificial intelligence [7−9] as shown in Figures 6.2 and 6.3.

Figure 6.1 Tuning and replication.
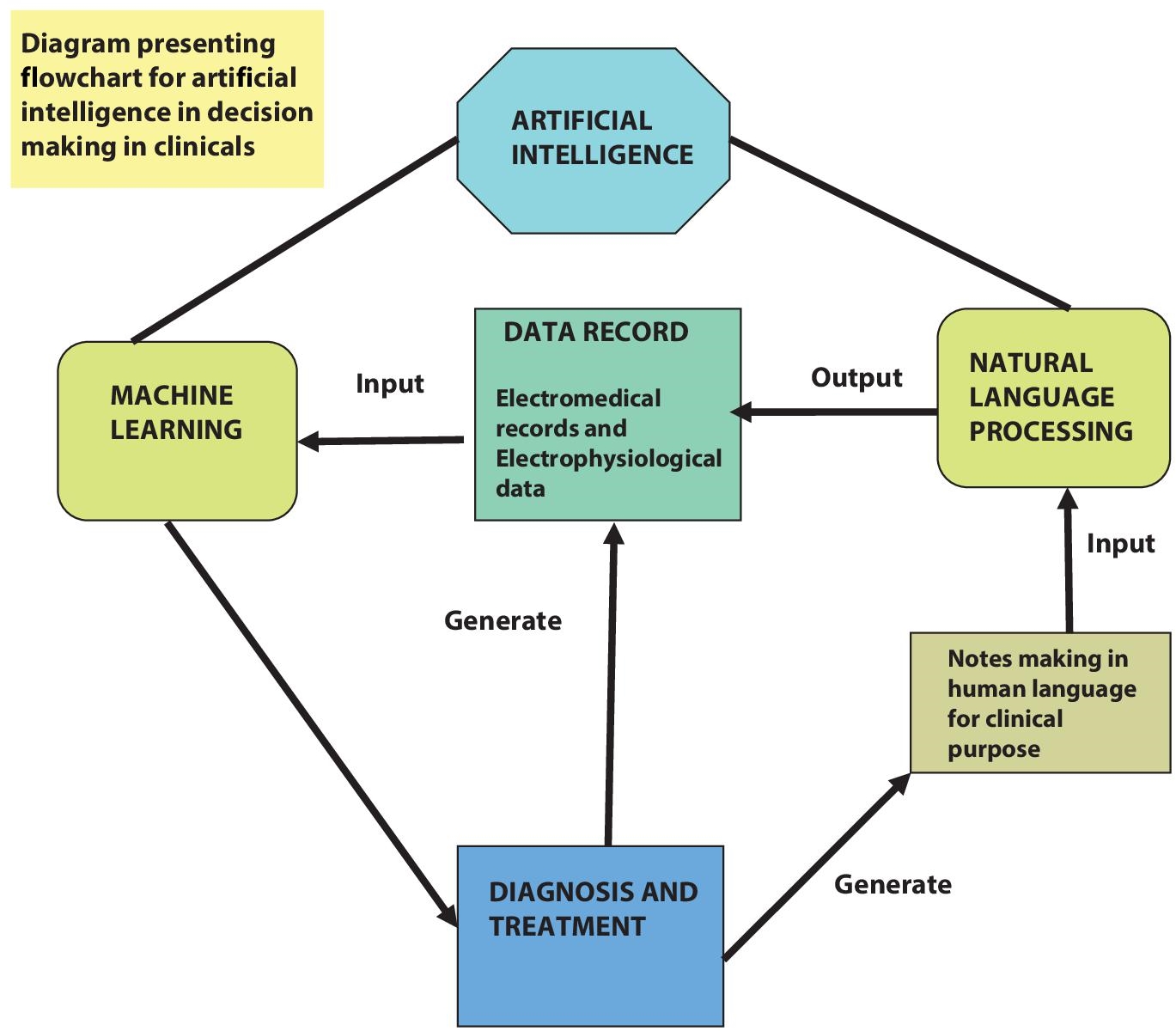
Figure 6.2 Application of artificial intelligence technology.
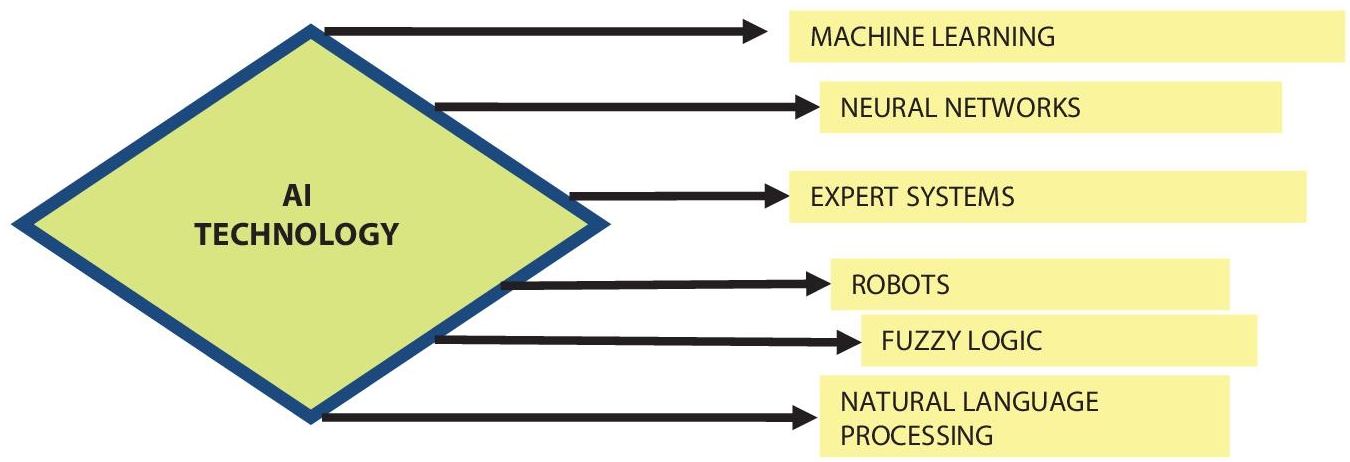
Figure 6.3 AI technologies.
6.2 Machine Learning
The concept of machine learning defines that where the machine learns to present as human and study their behavior, by this they can make the computer intelligent and make the progression of the artificial intelligence faster and precise towards accuracy. The concept of working machine learning travels similar by establishing the human cognitive skills, there thoughts, physiological changes at time of situation and emotional changes occurring at the same time. The significance of machine learning behind artificial intelligence is highly required to be intelligent, it should be consistent for being with learning capabilities. The machine learning itself is highly used in very diagnosis, medical procedures and many more technological works [10, 11].
The architecture behind the machine learning is the environment from where the learning abilities is gathered and the second it comes to learning which the most important factor to gather from environment and classify upon its completeness and incompleteness and quality. The third comes the knowledge base which affects the learning system by account of the expression such as reasoning, modification, presentation as shown in Figure 6.4. The last execution plays a wide role where it improves the learning skill by feedback, transparency and solves issues of complexity [12, 13].
There are types for machine learning algorithms as supervised learning where the expected output and the output came from computer is compared and the error is deleted to come up with expected one. The other is unsupervised where adaptation is done by exploring in the level of input cycle and this algorithm is also termed as cluster algorithm. The third is reinforcement learning where the actions are taken at environment level so as to improve long term output. The recommender systems are the customization process where the alteration is done as required by the usage [14].

Figure 6.4 Process architecture of machine learning.
6.3 Neural Networks
These are also known as artificial neural networks where they act as the neuron as present in human beings, as the function of neuron consisting of generating input signals from output signal and traveling after creation of threshold in building the bio-electrical signal passing through synapse, these function is also followed by the artificial neuron creating neuron network. The significance for the artificial neuron is to work as parallel processing, memory and signaling, and distributing equal data to every neuron [15, 16] as shown in Figure 6.5.
The structure of the artificial neuron is created with the development of 3 layers with different function such as input layer for input signals and names as “n” neurons whereas the intermediate layers is named after “m” neurons present with many intermediate and hidden channels and the output layers for the output signals and named after “p” neurons [17].
According to the feedback architecture of neural networks explaining the concept of the transferring the input signals as “x” and functioning the signal with “f ” and producing output as y, these layers are functional on each step according to the architecture but if there is no feedback architecture the signal will not be exchanged at every neuron but only be transferred to layers [18].

Figure 6.5 Artificial neural network.
6.4 Expert Systems
The expert systems act as the machine memory to enhance utility and provide better intellectual advice. They are solely depended on database large in size providing the justification and the specific knowledge in that context, as the creation of programs structured termed as knowledge based systems also as synonym to expert systems. Th provision of providing the knowledge to human is distinctive as gathered from books, as the information is such that as assembled in the specialists such as doctors, engineers, analysts and many more. The terms of knowledge depend on the level of interaction of the user and expert system. There are various technologies that are task specific to generate better outcomes which follows the rule as goal specific, better problem solving [19−21]. There are benefits behind experts systems are as better precision and accuracy than humans, more cheaper as in contrast to humans, better experience with success results, better in handling monotonous wok and increase expert skills, enable the compatibility with every system where humans aren’t, enhances the productive outcome. Nowadays the expert systems are more into the creation and maintaining the health records and manage it [22, 23]. The construction of expert system is flexible to represent the quantitative and qualitative measures, the knowledge base in the expert system is based on the equations working regarding the task where the there are letters headed in terms representing each such as force it as shear stress, D as data and diameter of coil, n is representation of number of coils involved. The rules engine consisting of the units such as length, diameter and other units which design the specific construction under these limited units. The data base present with number of designs which are compared to find and choose according to the optimal one as shown in Figure 6.6. The user interface is working in all long the process for creating a design and the expert makes it clear that is there any additional requirement as input. All this process finished the user provides advice for the application usage in this system [24, 25].
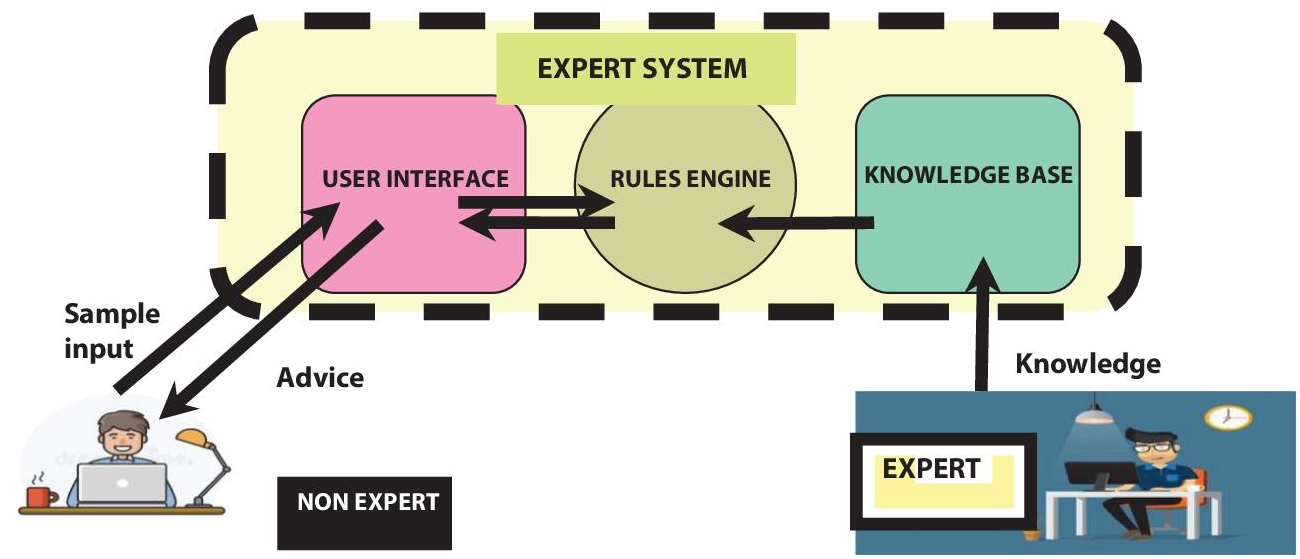
Figure 6.6 Working process of expert systems.
6.5 Robots
The robots are the new technology which are proven to be an assistant in human work with the combination of artificial technology the robots have been proven to be the essential in the rehabilitation and other healthcare approach as depicted in the figure below the artificial assistant with the assistive robot which is a source to the patient as attached with sensors gathering all the movements and the needs as sensors present at the patients wrist sending the signals to medical support, family and drafting the assistance with the help of robot turning as commuter and source for physical and social rehabilitation [26, 27].
In robotics there are two types, i.e., physical and social which plays role specifically , such as physical robots are for the cognitive, engaging to encourage to work and assist in activities of daily living, they are also specialized in surgery for the better precision and more coverage with limited exposure [28]. The other social robots are specially to play role in distinctive way such as social friend which pretends to be a coach to rehabilitate and instruct you to follow exercise protocol, play as a role to socialize, talk and be counsellor and allow to manage a psychologist with the human oriented intelligent technology as shown in Figure 6.7 [29−31].

Figure 6.7 Artificial intelligence with robotic system.
There are various benefits as allowing to create a feedback so as to come up with better outcome as with the support of the sensor technology the robots creates a data allowing the doctor to check the improvement and resolve the issue even if the patient is not reachable [32].
6.6 Fuzzy Logic
Fuzzy logic system is defined as technology for mathematics with engineering methodology which is changes the presentation of the human decision making as the difference between the yes and no and making various statements in between with variation [33]. The architecture system of the fuzzy logic work with models such as fuzzification as first where the signals of input are turn to five steps of differentiation from -2 to 2 with required term beside as used in distinct technologies as shown in Figure 6.8.
The second goes with rule setting which is done by the experts at the level of knowledge base. The third level moves to inference engine stimulating the signals to transform it to human reasoning turning from input. The fourth level moves to defuzzification where the fuzzy input is turn in to defuzzed output [34, 35].
The benefits of the fuzzy logic is to obtain easy decision making, better precision, fast conceptualization, making math understanding easier, working best in various fields of healthcare. There are some disadvantage such as works when the simple problems are there, no specific approach, and does not require high amount of accuracy [36, 37].
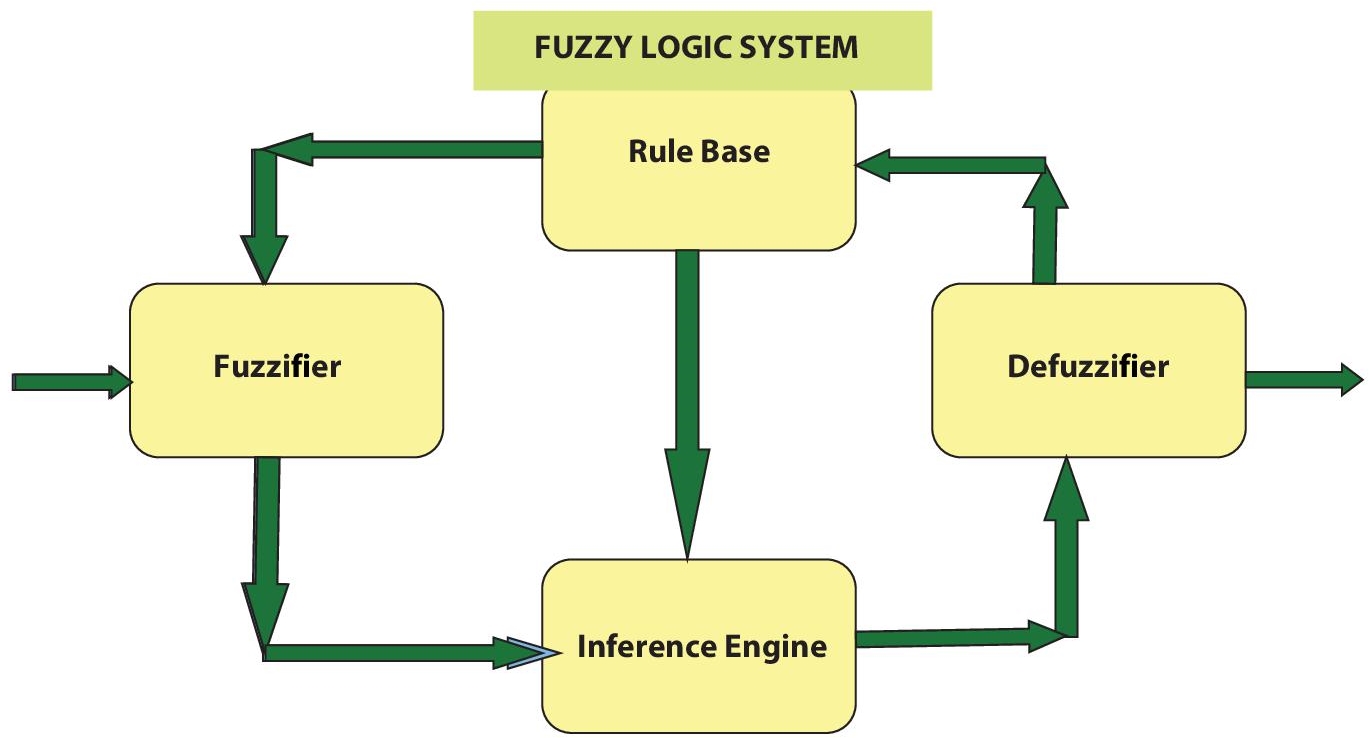
Figure 6.8 Fuzzy logic system.
The fuzzy logic plays a very less role which in artificial intelligence in healthcare where it plays the role of what human thinks and how they judge and provide the feedback , accordingly the fuzzy logic follows [38].
6.7 Natural Language Processing
Natural language processing (Figure 6.9) is that part of the artificial intelligence playing the role in linguistics, where the computer tries to process the computer language in normal human language so as to make understanding clear in all aspects of different human language making understood by other person who is unable to go through different languages [39, 40].
Natural language processing is composed of various components that make the architecture of the concept better, it is present with term known as phonology that id defined as making arrangement to create a sound that is systematic that is a study of obtaining the sounds and study the sound language, The others is morphology that is defined as the nature of letters and words presenting the morpheme which is in nature that it cannot be divided. Lexical the component which provided the meaning to the words and multiple parts of speech as required in the context, this can be variable according to semantic theory. The syntactic component is for the grammar presentation, as by keeping the sentence structure and equality among the words and their relation. The semantic component provides the meanings according to the level of sentence incorporation and presenting in different parts of speech. The discourse component work to keep the length of the sentence as required and making it structural. The pragmatic component provides better usage of words in the sentences and providing nub so as to get other meanings from the same sentence [41−44].
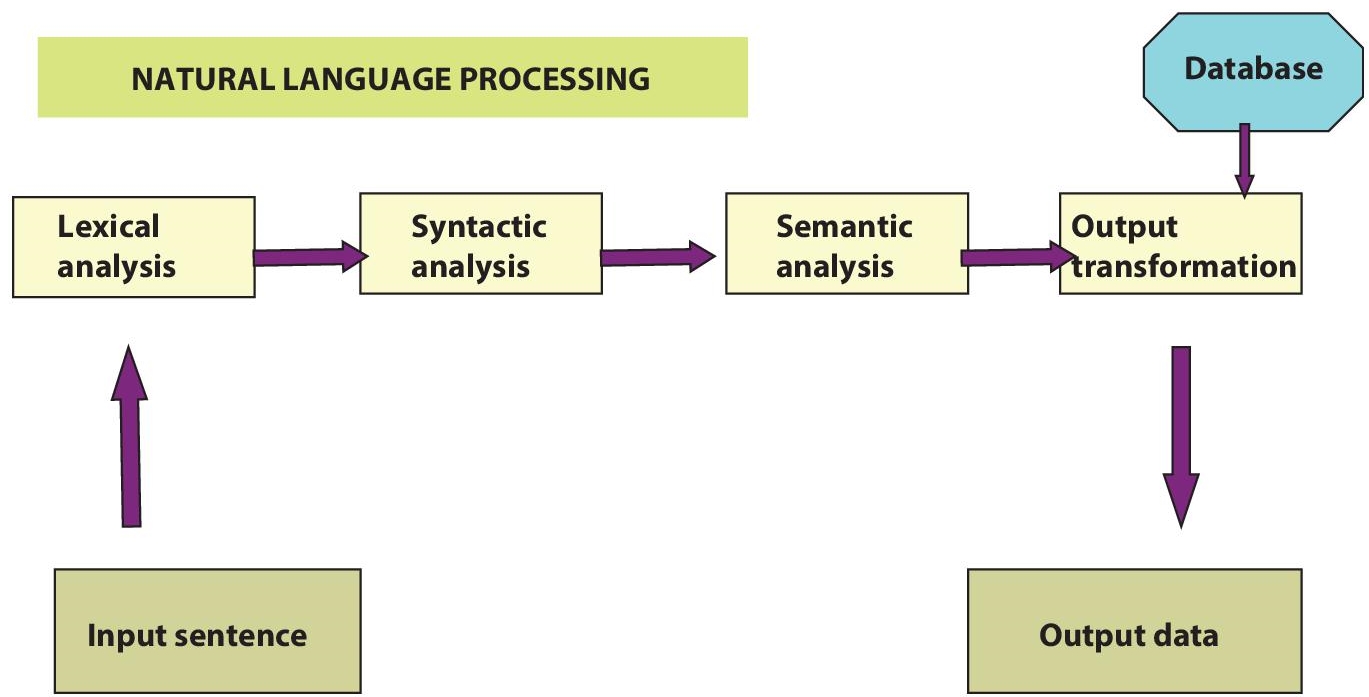
Figure 6.9 Language processing system.
The generation takes place with speaker and generator in which the phrase is generated according to the user intention. The components for generation will be including of selection of the context to organization of the material to the source for lingual clarity and then realizing for the outcome, then in last the application and the speaker will be done according to the situation [45].
6.8 Sensor Network Technology in Artificial Intelligence
There are various wireless sensors that play the role in artificial intelligence to just same as the sensory system present in the humans as same as in intelligent computers there are sensory networks, modern sensors, sensory architecture in artificial intelligence [46–48].
The sensory networks are wireless connection that are connected in the computer system such as the bunch of nerves in limbs of human, this is required so as for the place where the wires cannot be deployed such as withe patient while doing activity so as to record the activity, military combat zone, geology places and many more, these are utilized in parameter systems to automatically measure such as by spatial and temporal environment [49, 50].
The modern sensors are in sensory networks with the advancement in better compatibility as with the process of nanotechnology as thousands of sensors are applied in sensory nodes which gathers even a small change and notifies the intelligent computer. They work on qualitative and quantitative in nature such as precision, accuracy, low cost, easy availability and require less energy for the same as shown in Figure 6.10. These sensors are proven to be best for the aspect of environment, communication and easily made by the satellite connection so can be used in area as being wireless [51−53].
Architecture of Sensory Network
The sensory network is mesh space with number of nodes which are point to point in relation where it accesses the geographical measures and where kept. This mesh does not require the transmitter to signal ad transfer the information as this is having ability to transfer on its own as the nodes are so close in the sensors. The network is equally distributed and placed so as extract, collect and synthesize the data. The data is centrally sent to the nodes to create one center data, due to this the sensors are having the self-configuration that increases its capability. The advantage of this structure is there is no dependency to repeat, better expanding property. The disadvantage is the battery consumption and the signal should be passed from every node [54, 55].
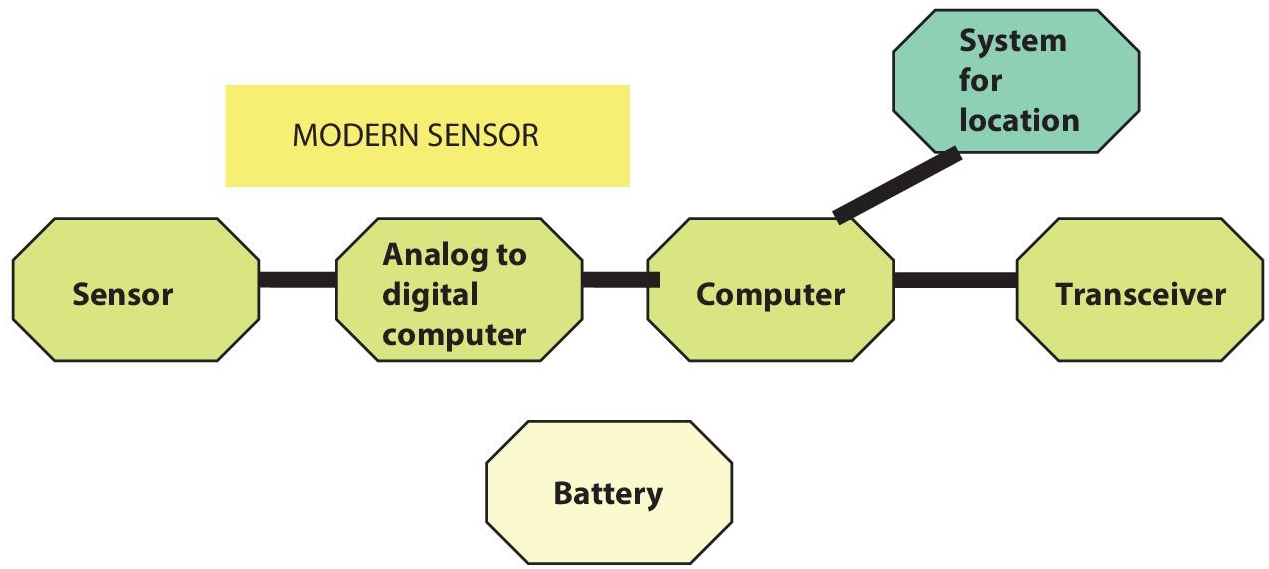
Figure 6.10 Sensor network system.
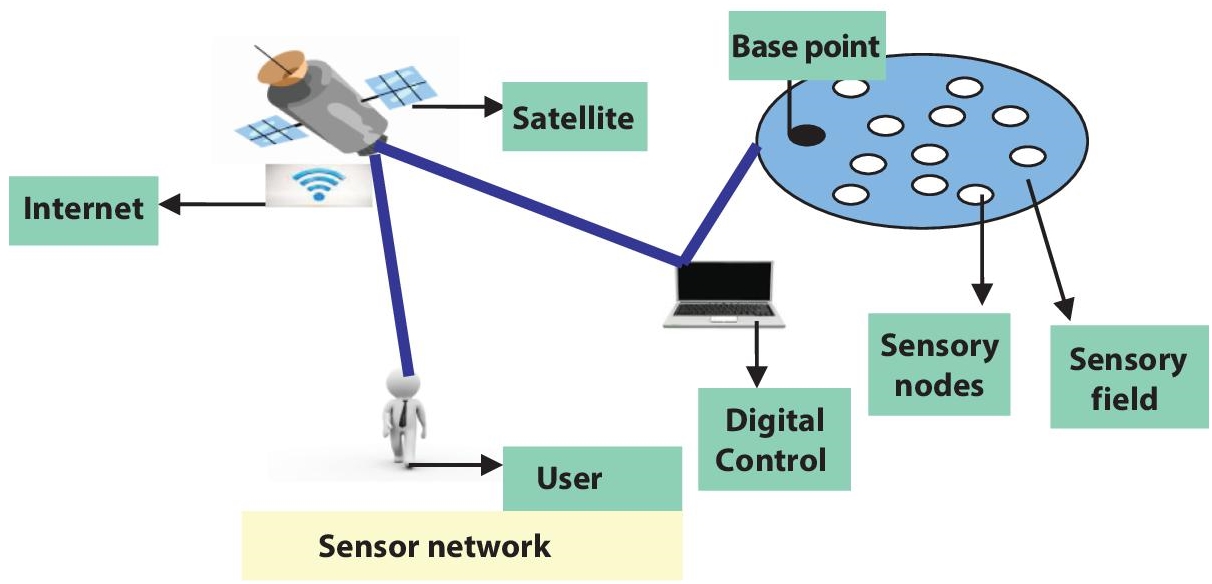
Figure 6.11 Sensor network system.
The sensory network architecture is both with static and mobility in nature where the nodes that power to find the exact place of themselves even when distributed unevenly and they are once processed through authentication once employed in work. The nodes are present with ability to store the memory up to hundreds of bytes with the help of cryptography system. There are two points one is key server and other is base station which is connected to laptops and can be controlled through wireless networks as shown in Figure 6.11 [56, 57].
6.9 Sensory Devices in Healthcare
There are basically two types of sensor in healthcare one is wearable and other is implanted and there are energy harvesters that are applied respectively. These devices are quite flexible and soft in nature providing the relation between the device and human and enhancing the output. There are devices which are nowadays researched and made the sensor to be charged by the human contact which can be acted as the energy harvesters [58−61].
6.9.1 Wearable Devices
The wearable devices are such that it works by epidermis and act as e skin which have the property to be as human interaction interface resulting in generation of bio-metric signals which records the acoustic and mechanical signals in the in the body and turns into feedback such as recording heart rate, murmurs, temperature [62−65]. Wearable devices are present with the noninvasive quality hence accepted fast by the patients. There are mechanisms through which the transfer leading to outcome such as piezzo-electric mechanism where there are fine sheets or wires in the sensors which is transmitting the mechanical energy to electrical energy for output, the other is thermo electric mechanism where the temperature is the transmitter for turning the output into electrical energy, triboelectric mechanism where there is the coupling mechanism of the and having triboelectric nanogenerator where the signals are transferred through fabrics and polymer [66−72].
6.9.2 Implantable Devices
These are the devices that are to be placed inside the body which is having main function to stimulate the muscle or organ such as in case of deep brain stimulation which generate or stop the signal so as to control the tremors and pain by controlling the brain signals, it can also be used as the pacemaker in the heart so as to generate the heart signals to pump the heart. These devices are also used to deliver the drug at equal intervals as they are somewhat battery oriented in some device and some as present with the energy harvesters [73−76]. According to the study , as the external power supply is the problem for the implantable device hence can be adjusted and combined with wearable device so as to interact the neural interface and generate the power by different mechanism, such as muscle stimulation, temperature gradient, and use of ultra violet rays that interacts with E skin and leading to power supply without the use of battery. The energy harvesters are like zinc oxygen single wire generator gets triggered by the human heart beat, blood pressure and generates the biomechanical energy to electrical energy. There are also piezo nano-wires that also work on the same principle with the physical vapor deposition technique [77−82].
6.10 Neural Interface for Sensors
The neural interface is between the sensor and the human body interaction where the interaction can be with central nervous system and peripheral nervous system. The study for the nervous system is still difficult to rule out the outcomes and still the research is under procedure [83−86]. The neural interface for central nervous system is for brain, scalp and cortical surface which generates signals which are as the electroencephalogram, electrocorticogram, and local end potential respectively where the electrodes and sensors are placed according to depth so as to get the graph for the same (Figure 6.12). Now the flexibility of the sensors have increased leading to better implantation and better neural interface such as technique of optoelectronic interface through optoelectronic implants, syringe implanted mesh electronics, micro needle electrodes and E dura implant for spinal cord [87−89].
For peripheral nervous system the signaling is from the head to the branches for communication the devices are different such as transverse intrafasicular multi-channel electrode, flat interface nerve electrode, 3D spike ultraneural interface, these all interface communicates through the sensory system and transmitting signals from and to high authorities. This can be useful in case of neuroprosthesis, and nerve stimulation according to the condition (Figure 6.13) [90−94].
6.10.1 Intrusion Devices in Artificial Intelligence
The wireless sensory networks are very useful in all the ways, but there is only the risk of safety and privacy which needs to be taken care for. Hence there are various safety mechanisms but not energy beneficial; hence, the researchers came to the intrusion systems that are possible solution for the safety aspects. The intrusion systems are flexible in determining the problems and safety attacks but are unable to diffuse it. There are basically three types of intrusion system that are coping the human system such as the artificial immune intrusion device exactly works as human immunity, the artificial neural networks intrusion works as neurons and genetic intrusion works on the biological criteria of humans [95−98].

Figure 6.12 Sensor-based healthcare devices.
The artificial immune intrusion devices are the scanners for upcoming threat same as our D cells T cells and B cell work. The architecture for the artificial systems works as the ruling out the database, monitoring for the logs, checking for the traffic and ruling for the type of attack and alarming and responding accordingly [99−101].
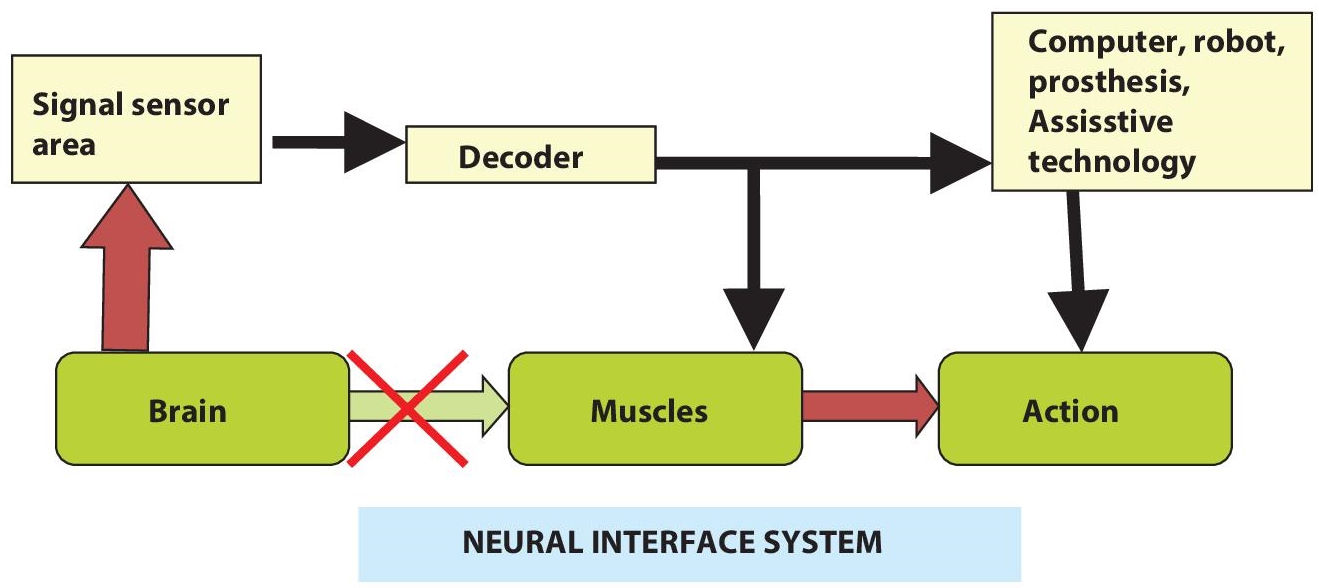
Figure 6.13 Neural interface system.
The artificial neural networks intrusion devices are same as connection of nervous system with neurons, where the artificial neural networks will be capable of identifying for the complex trends. The feed-forward ANN working only in one direction whereas the feedback moves in all direction, here the intrusion devices rule out the normal and abnormal events, determining the exhaustion attacks. Once the attack is identified the robot behind works for the same [102−104].
Genetic algorithms intrusion devices are best for computing solutions, adaptive in nature and for solving the problem. This works on the concept selection naturally, evolution, and mutation theory and inherited genes as in humans. It is useful in intrusion by creating the design and proposition and classifying the rule of attacks and produce new rules to satisfy the attack prevention [105, 106].
6.11 Artificial Intelligence in Healthcare
6.11.1 Role of Artificial Intelligence in Medicine
The medicine is major field of healthcare as nowadays the level of knowledge is increasing so as the level of research hence leading to wide amount of challenges such as adapting, implementing, and analyzing the challenges this where the modern medicine occur which requires artificial intelligence to solve the specialists and physician to resolve by formulation and variable diagnosis [107−110].
The artificial neural networks plays the role as the human nervous system consisting of neurons which analyze, drafts the easier method of changes in more presentable and understanding analytics keeping the data in order and productive. The neural networks work in diagnosis such as in radiology and histopathology with the help of deep analysis and analytical and data presentation such as PAPNET specifically for cervical examination and screening. ANN can interpret all the radiology sheets from plain to MRI and plain graphs from ECG to EEG too. The prognosis is also made very fast and accurate by the neural networks and outcome is interpreted even before and after surgery [111−119].
The fuzzy systems in the medicine plays the role by giving the variation to the medical diagnosis not just by yes or no and black and white but also classification in between them to precise and accurate the results and differentiate the diagnosis. It works best in imaging such as ultrasound, computed tomography and magnetic reasoning imaging [120, 121].
According to the study there is a new concept of the hybrid intelligent system where the there is a relation with artificial neural networks , fuzzy expert system and genetic algorithm which in combination will make the medicine department to another level of outcome with better assessment and outcome and through which prognosis will be easier to be encouraged [122−124].
6.11.2 Role of Artificial Intelligence in Surgery
The artificial intelligence plays the role in surgery by better recognition, cognitive ability, and decision making.
Machine learning in surgery works as predictor and patter recognizer to machines. The machine learning enables to structure to the detected data and predict the programming according to that. It is having the ability to conceptualize the predictive outcomes and, hence can be alarming at the time of surgery. It is developed with multiple algorithms facility that makes it more convenient to statistically present. Natural language processing has the ability to process in the human language. In surgical purpose the natural language processing is used as the comb to utter all the electrical medical records and maintain the language according to surgeon. This makes surgeon to be sure whatever is he doing is exact with the assessment and the NLP generates the condition of the patient according to the situation in the theater. Artificial neural networks helps to classify the data, manage the complex surgery with the problems to be in pattern [125−128].
6.11.3 Role of Artificial Intelligence in Rehabilitation
In rehabilitation the robots work as artificial intelligence where the role of combination works such as sensors, robotic technology and the processing behind as the role of the artificial intelligence can be through virtual, robotic or sensory feedback to the environment linking your day to day activities and charting accordingly, where the robot can act as the trainer, care taker, motivator which in together progress to rehabilitation the devices such as endoskeleton, exoskeleton, and MIT manus are the technology behind it [129−131].
6.12 Why Artificial Intelligence in Healthcare
The artificial intelligence is accepted due to the curation of the data as the basic problem nowadays is absent data that makes difficult to analyze and bring out the documentation as for what and how the diagnosis, prognosis can be manipulated so as to gather the information worldwide [132].
It is required due to presence with management of strategic change in the capacity, as the procedure of the artificial intelligence is not only to reach with algorithmic solutions but also to make aware in healthcare professionals and try with the trials and draw the outcomes which can be easily compared by the data collection and presentation in the device [133].
It plays a great role in accountability by creating thousands of classifications and that will and multiple algorithms where according to the law the explanation is the term for the solution to every problem and justify accordingly, where the accountability for this occurs [134].
The priority of the artificial intelligence comes as the privacy and data management where the data is to be kept in private as the data involves national statistical data which interprets the level of the nation, hence it is secured with the safety guards oriented by side and organization creating the procedure under artificial intelligence [135].
6.13 Advancements of Artificial Intelligence in Healthcare
According to the data reported in a study interprets that the artificial intelligence is the most benefiting in terms for the healthcare systems, there are very recent advances that place a very decent role in healthcare systems.
The role in mobile health where the wireless technologies are grasped by the patient and creates the innovative idea by keeping the health record in hand always wherever and whenever, as the awareness towards the smart phones and fitness is increasing leading to increase in mobile applications not even in patients but in normal person to so s to keep a record and motivate and encourage themselves according the outcome and feedback of daily living. The mobile applications not only help to keep a record but to plan for the further days and keep the genuine record for the medical professional to keep an eye towards his patient [136, 137].
The role of artificial intelligence have come up so far with the technology of keeping the electro medical records which are private healthcare information of every patient in every visit and type of management provided by every healthcare professional. As the data storage s quite high and the prevalence of low resource is there hence the electro medical records can act as placed with multiple safety guards preventing and creating the suitable treatment for the particular condition [138, 139].
The storage devices are quite less and heavy to store hence the information technology have come up with the concept of cloud computing which is secured by the passwords and linked with the accounts as any mishap happens will be on the spot complained, as this will be the matter of security in public health [140].
6.14 Future Challenges
The future challenges are eye opener to artificial intelligence as the points to be covered under the research for the healthcare ad artificial intelligence. The great challenge is the acceptance and adoption the feature for the society of every category according to availability, financially and can be accepted in the large area of scale. The myth to be removed as thought by the people of the society as the technology can remove the healthcare professionals. To come up with the results it will take accordingly 5 to 10 years to overcome and challenge the further challenge on every step [141, 142].
6.15 Discussion
According to the data studied and reviewed interprets the technology of the artificial intelligence, its working, mechanism of machine learning, natural language processing, fuzzy logics, robots, expert system, artificial neural networks where these mechanism ought to act same as the human system of working from cognitive, decision making, action of nervous system, expert mind setting and in terms of memory [143, 144].
According to the study the artificial intelligence is a successful technology with benefits for healthcare sectors specific to medicine, surgery, rehabilitation, and even more specific to the subjects below it such as cardiology, neurology, oncology, orthopedics and many more. The technology is not limited to the treatment but also validated towards all the administration in private, public and community healthcare sectors where the data security, accountability and data presentation is to rectify in case of the experimental trials. This technology gives rise to suitability of research to wide place and accountability towards the sector. The intelligent not only copies the language, areas but also takes the image for the decision according to humans and society which in turns better outcomes [145−147].
6.16 Conclusion
This study concluded with the effects of the artificial intelligence and its potential ability in the healthcare sector and be a hand for healthcare professionals. It can be beneficial in all aspects of healthcare sectors with its different technologies and very structural in aspects of results and outcomes by creation of real data presentation. The AI is motivator for the healthcare sector not the remover for the professionals.
References
- 1. Frankish, K. and Ramsey, W.M. (Eds.), The Cambridge Handbook of Artificial Intelligence, United States of America by Cambridge University Press, New York, 2014.
- 2. Poole, D.L. and Mackworth, A.K., Artificial Intelligence: Foundations of Computational Agents, United States of America by Cambridge University Press, New York, 2010.
- 3. Yu, K.-H., Beam, A.L., Kohane, I.S., Artificial intelligence in healthcare. Nat. Biomed. Eng., 2, 719–731, 2018.
- 4. Trivikram, C., Samarpitha, S., Madhavi, K., Moses, D., Evaluation of hybrid face and voice recognition systems for biometric identification in areas requiring high security. I-Manag. J. Pattern Recognit., 4, 9–16, 2017.
- 5. Hamet, P. and Tremblay, J., Artificial intelligence in medicine. Metabolism, 69, S36–S40, 2017.
- 6. Tran, B.X., Vu, G.T., Ha, G.H., Vuong, Q.H., Ho, M.T., Vuong, T.T., La, V.P., Ho, M.T., Nghiem, K.P., Nguyen, H., Latkin, C.A., Tam, W., Cheung, N.M., Nguyen, H.T., Ho, C., Ho, R., Global evolution of research in artificial intelligence in health and medicine: A bibliometric study. J. Clin. Med., 8, 3, 360, 2019.
- 7. Begovic, M., Oprunenco, A., Sadiku, L., Let’s Talk about Artificial Intelligence, vol. 2019, UNDP, New York, NY, USA, 2018.
- 8. Jiang, F., Jiang, Y., Zhi, H., Dong, Y., Li, H., Ma, S., Wang, Y., Dong, Q., Shen, H., Wang, Y., Artificial intelligence in healthcare: Past, present and future. Stroke Vasc. Neurol., 2, 230–243, 2017.
- 9. Shaban-Nejad, A., Michalowski, M., Buckeridge, D.L., Health intelligence: How artificial intelligence transforms population and personalized health. NPJ Digit. Med., 1, 53, 2018.
- 10. Springhead, W. and Jiang, L., Artificial Intelligence and Expert System, vol. 160-180, pp. 277–280, National University of Defense Technology Publishing House, 1995.
- 11. Yongqing, W., Expert System WMES Research and Realization, vol. 6, pp. 14–15, The Microcomputer Develops, Springer, 1994.
- 12. Yangsen, Z., Artificial Intelligence Principle and Application, Higher Education Publishing House, 2004.
- 13. Xue, M. and Zhu, C., A study and application on machine learning of artificial intelligence, in: 2009 International Joint Conference on Artificial Intelligence, IEEE, pp. 272–274, April 2009.
- 14. Das, S., Dey, A., Pal, A., Roy, N., Applications of artificial intelligence in machine learning: Review and prospect. Int. J. Comput. Appl., 115, 9, 31–41, 2015.
- 15. Honkela, T., Duch, W., Girolami, M., Kaski, S. (Eds.), vol. 6792, Artificial Neural Networks and Machine Learning-ICANN 2011: 21st International Conference on Artificial Neural Networks, Proceedings, Espoo, Finland, Springer June 14-17, 2011.
- 16. Gallo, C., Artificial neural networks tutorial, in: Encyclopedia of Information Science and Technology, Third Edition, pp. 6369–6378, IGI Global, 2015.
- 17. McCulloch, W.S. and Pitts, W., A logical calculus of the ideas immanent in nervous activity. Bull. Math. Biophys., 5, 4, 115–133, 1943.
- 18. Hornik, K., Stinchcombe, M., White, H., Multilayer feedforward networks are universal approximators. Neural Netw., 2, 5, 359–366, 1989.
- 19. Horvitz, E.J., Breese, J.S., Henrion, M., Decision theory in expert systems and artificial intelligence. Int. J. Approx. Reason., 2, 3, 247–302, 1988.
- 20. Sol, H.G., Cees, A.T., de Vries Robbé, P.F. (Eds.), Expert Systems and Artificial Intelligence in Decision Support Systems: Proceedings of the Second Mini Euroconference, Lunteren, Springer Science & Business Media, The Netherlands, November 17–20, 1985, 2013.
- 21. Patterson, D.W., Introduction to Artificial Intelligence and Expert Systems, Prentice-Hall, India, 1990.
- 22. Vial, A., Stirling, D., Field, M. et al., The role of deep learning and radiomic feature extraction in cancer-specific predictive modelling: A review. Transl. Cancer Res., 7, 803–16, 2018.
- 23. Krishnamoorthy, C.S. and Rajeev, S., Artificial Intelligence and Expert Systems for Engineers (Vol. 11), CRC Press, 1996.
- 24. Alty, J.L. and Coombs, M.J., Expert Systems: Concepts and Examples, OSTI Gov U.S. Department of Energy Officeof Scientific and Technical Information, 1984.
- 25. Duda, R.O. and Shortliffe, E.H., Expert systems research. Science, 220, 4594, 261–268, 1983.
- 26. van den Heuvel, R.J., Lexis, M.A., Gelderblom, G.J., Jansens, R.M., de Witte, L.P., Robots and ICT to support play in children with severe physical disabilities: A systematic review. Disabil. Rehabil. Assist. Technol., 11, 2, 103–116, 2016.
- 27. Riek, L.D., Healthcare robotics. Commun. ACM, 60, 11, 68–78, 2017.
- 28. Hussain, A., Malik, A., Halim, M.U., Ali, A.M., The use of robotics in surgery: A review. Int. J. Clin. Pract., 68, 1376–82, 2014.
- 29. Kraft, K., Chu, T., Hansen, P., Smart, W.D., Real-time contamination modeling for robotic healthcare support, in: 2016 IEEE/RSJ International Conference on Intelligent Robots and Systems (IROS), IEEE, pp. 2249–2254, October 2016.
- 30. Luxton, D.D. and Riek, L.D., Artificial intelligence and robotics in rehabilitation, APA Psycnet, 2019.
- 31. Tapus, A. and Mataric, M.J., Emulating empathy in socially assistive robotics, in: AAAI Spring Symposium: Multidisciplinary Collaboration for Socially Assistive Robotics, pp. 93–96, March 2007.
- 32. Davenport, T.H. and Glaser, J., Just-in-time delivery comes to knowledge management. Harv. Bus. Rev., 80(7):107-11, 126, 2002.
- 33. Dubois, D. and Prade, H., Fuzzy Sets and Systems: Theory and Applications, Academic Press, New York, 1980.
- 34. Biradar, A., Fuzzy Logic System in Artificial Intelligence, International Journal of Advance Research in Science, Engineering and Technology, advance journal publications, 2016.
- 35. Mendel, J., Fuzzy logic systems for engineering: A tutorial. Proc. IEEE, 83, 345–377, 1995.
- 36. Fraleigh, S., Fuzzy logic and neural networks: Practical tools for process management. PC AI, 8, 3, 16–21, 1994.
- 37. Tanaka, K., An Introduction to Fuzzy Logic for Practical Applications, Springer, 1997.
- 38. Cavus, N., The evaluation of Learning Management Systems using an artificial intelligence fuzzy logic algorithm. Adv. En. Software, 41, 2, 248–254, 2010.
- 39. Rospocher, M., van Erp, M., Vossen, P., Fokkens, A., Aldabe, I., Rigau, G., Soroa, A., Ploeger, T., Bogaard, T., Building event-centric knowledge graphs from news. Web Semant. Science, Serv. Agents World Wide Web, In Press, 37–38, 2016, 132–151, 2016.
- 40. Shemtov, H., Ambiguity Management in Natural Language Generation, Pennsylvania State University, Stanford, 1997.
- 41. Nation, K., Snowling, M.J., Clarke, P., Dissecting the relationship between language skills and learning to read: Semantic and phonological contributions to new vocabulary learning in children with poor reading comprehension. Adv. Speech Lang. Pathol., 9, 2, 131–139, 2007.
- 42. Liddy, E.D., Natural language processing, Syracuse University, 2001.
- 43. Feldman, S., NLP Meets the Jabberwocky: Natural Language Processing in Information Retrieval, vol. 23, pp. 62–73, ONLINE-WESTON THEN WILTON-, Eric education, 1999.
- 44. Kumar, A., Irsoy, O., Ondruska, P., Iyyer, M., Bradbury, J., Gulrajani, I., Socher, R., Ask me anything: Dynamic memory networks for natural language processing, in: International Conference on Machine Learning, pp. 1378–1387, June 2016.
- 45. Natural Language Processing, Natural Language Processing RSS, Web. Mar. Capturing the patient’s perspective: A review of advances in natural language processing of health-related text. Yearbook of medical informatics, 26(01), 214–227, 2017.
- 46. Volosencu, C., Identification of distributed parameter systems, based on sensor networks and artificial intelligence. WSEAS Trans. Syst., 7, 785–801, 2008.
- 47. Banks, H.T. and Kunish, K., Estimation Techniques for Distributed Parameter Systems, Systems & Control: Foundation & Applications, vol. 1, pp. Note(s): XIII–315, Wiley online library, 1989.
- 48. Volosencu, C. et al., Malicion node detection in sensor network using autoregression based on neural network. 4th IFAC Conf. on Management and Control of Production and Logistics, MCPL2007, Sibiu, pp. 571–577, 2007.
- 49. Volosencu, C., Curiac, D.I., Doboli, A., Dranga, O., Knowledge based system for reliable perimeter protection using sensor networks. Int. Conf. Winsys 2007, Barcelona, 2007.
- 50. Krishnamachari, B., A Wireless Sensor Networks Bibliography, Technical Report, University of Southern California, 2007.
- 51. Akyildiz, I.F., Su, W., Sankarasubramaniam, Y., Cayirci, E., Wireless sensor networks: A survey. Comput. Netw., 38, 4, 393–422, March 2002.
- 52. Tubaishat, M. and Madria, S., Sensor networks: An overview. IEEE Potentials, 22, 2, 20–23, Apr. 2003.
- 53. Demetriou, M.A., Adaptive identification of second-order distributed parameter systems. Inverse Probl., 10, 261–294, 1994.
- 54. Krishnamachari, B., A Wireless Sensor Networks Bibliography, Technical Report, University of Southern California, 2007.
- 55. Feng, J., Koushanfar, F., Potkonjak, M., System architectures for sensor networks issues, alternatives and directions. Proc. of the 2002 IEEE Int. Conf. on Computer Design (ICCD’02), Freiburg, pp. 226–231, 2002.
- 56. Volosencu, C., Identification of distributed parameter systems based on sensor networks, in: New Trends in Technologies: Control, Management, Computational Intelligence and Network Systems, pp. 369–394, 2010.
- 57. Volosencu, C., Identification of distributed parameter systems, based on sensor networks and artificial intelligence. Methods, 13, 17, 2008.
- 58. Bariya, M., Nyein, H.Y.Y., Javey, A., Wearable sweat sensors, Nat. Electron., 1, 3, 160–171, 2018.
- 59. Lissandrello, C.A., Gillis, W.F., Shen, J., Pearre, B.W., Vitale, F., Pasquali, M., Holinski, B.J., Chew, D.J., White, A.E., Gardner, T.J., A micro-scale printable nano clip for electrical stimulation and recording in small nerves, J. Neural Eng., 14, 3, 036006, 2017.
- 60. Osborn, L.E., Dragomir, A., Betthauser, J.L., Hunt, C.L., Nguyen, H.H., Kaliki, R.R., Thakor, N.V., Prosthesis with neuromorphic multilayered e-dermis perceives touch and pain, Sci. Robot., 3, 19, eaat3818, 2018.
- 61. Raspopovic, S., Capogrosso, M., Petrini, F.M., Bonizzato, M., Rigosa, J., Di Pino, G., Carpaneto, J., Controzzi, M., Boretius, T., Fernandez, E., Granata, G., Oddo, C.M., Citi, L., Ciancio, A.L., Cipriani, C., Carrozza, M.C., Jensen, W., Guglielmelli, E., Stieglitz, T., Rossini, P.M., Micera, S., Restoring natural sensory feedback in real-time bidirectional hand prostheses. Sci. Transl. Med., 6, 222, 222ra219, 2014.
- 62. Kim, D.H., Lu, N., Ma, R., Kim, Y.S., Kim, R.H., Wang, S., Wu, J., Won, S.M., Tao, H., Islam, A., Yu, K.J., Kim, T., II, Chowdhury, R., Ying, M., Xu, L., Li, M.L., Chung, H.J., Keum, H., McCormick, M., Liu, P., Zhang, Y.W., Omenetto, F.G., Huang, Y., Coleman, T., Rogers, J.A., Epidermal electronics, Science, 333, 838, 2011.
- 63. Chortos, A., Liu, J., Bao, Z., Pursuing prosthetic electronic skin, Nat. Mater., 15, 9, 937–950, 2016.
- 64. Rezai, A.R., Phillips, M., Baker, K.B., Sharan, A.D., Nyenhuis, J., Tkach, J., Henderson, J., Shellock, F.G., Neurostimulation system used for deep brain stimulation (DBS): MR safety issues and implications of failing to follow safety recommendations. Invest. Radiol., 39, 5, 300–303, 2004.
- 65. Horch, K.W. and Dhillon, G.S., Neuro prosthetics-Theory and practice, World Scientific Publishing Co. Pte. Ltd, 2004.
- 66. Park, K., II, Lee, M., Liu, Y., Moon, S., Hwang, G.T., Zhu, G., Kim, J.E., Kim, S.O., Kim, D.K., Wang, Z.L., Flexible nanocomposite generator made of BaTiO3 nanoparticles and graphitic carbons. Adv. Mater., 24, 22, 2999–3004, Wiley online library, Deerfield Beach, Fla., 2012
- 67. Jeong, C.K., Lee, J., Han, S., Ryu, J., Hwang, G.T., Park, D.Y., Park, J.H., Lee, S.S., Byun, M., Ko, S.H., Stretchable piezoelectric nanocomposite generator. Adv. Mater., 27, 18, 2866–2875, 2015.
- 68. Park, K.-I., Jeong, C.K., Ryu, J., Hwang, G.-T., Lee, K.J., Flexible and largearea nanocomposite generators based on lead zirconate titanate particles and carbon nanotubes, Adv. Energy Mater., 3, 12, 1539–1544, 2013.
- 69. Zhu, G., Yang, R., Wang, S., Wang, Z.L., Flexible high-output nanogenerator based on lateral ZnO nanowire array, Nano Lett., 10, 8, 3151–3155, 2010.
- 70. Fattahi, P., Yang, G., Kim, G., Abidian, M.R., Replacing a battery by a nanogenerator with 20 V output, Adv. Mater., 26, 12, 1846–1885, 2014.
- 71. Qi, Y., Kim, J., Nguyen, T.D., Lisko, B., Purohit, P.K., McAlpine, M.C., Enhanced piezoelectricity and stretchability in energy harvesting devices fabricated from buckled PZT ribbons, Nano Lett., 11, 3, 1331–1336, 2011.
- 72. Hwang, G.T., Annapureddy, V., Han, J.H., Joe, D.J., Baek, C., Park, D.Y., Kim, D.H., Park, J.H., Jeong, C.K., Park, K., II, Self‐powered wireless sensor node enabled by an aerosol‐deposited PZT flexible energy harvester, Adv. Energy Mater., 6, 13, 1600237, 2016.
- 73. Lee, S., Wang, H., Wang, J., Shi, Q., Yen, S.-C., Thakor, N.V., Lee, C., Battery-free neuromodulator for peripheral nerve direct stimulation, Nano Energy, 50, 148–158, 2018.
- 74. Hwang, G.T., Kim, Y., Lee, J.H., Oh, S., Jeong, C.K., Park, D.Y., Ryu, J., Kwon, H., Lee, S.G., Joung, B., Kim, D., Lee, K.J., Self-powered deep brain stimulation via a flexible PIMNT energy harvester, Energy Environ. Sci., 8, 9, 2677– 2684, 2015.
- 75. Lee, S., Wang, H., Shi, Q., Dhakar, L., Wang, J., Thakor, N.V., Yen, S.-C., Lee, C., Development of battery-free neural interface and modulated control of tibialis anterior muscle via common peroneal nerve based on triboelectric nanogenerators (TENGs), Nano Energy, 33, 1–11, 2017.
- 76. Ravi, S.K., Wu, T., Udayagiri, V.S., Vu, X.M., Wang, Y., Jones, M.R., Tan, S.C., Photosynthetic bioelectronic sensors for touch perception, UV-detection and nanopower generation: Toward self-powered e-skins, Adv. Mater., 30, 39, e1802290, 2018.
- 77. Hwang, G.T., Park, H., Lee, J.H., Oh, S., Park, K., II, Byun, M., Park, H., Ahn, G., Jeong, C.K., No, K., Self-powered cardiac pacemaker enabled by flexible single crystalline PMN-PT piezoelectric energy harvester, Adv. Mater., 26, 28, 4880–4887, 2014.
- 78. Dagdeviren, C., Yang, B.D., Su, Y., Tran, P.L., Joe, P., Anderson, E., Xia, J., Doraiswamy, V., Dehdashti, B., Feng, X., Lu, B., Poston, R., Khalpey, Z., Ghaffari, R., Huang, Y., Slepian, M.J., Rogers, J.A., Conformal piezoelectric energy harvesting and storage from motions of the heart, lung, and diaphragm, Proc. Natl. Acad. Sci. U. S. A., 111, 5, 1927–1932, 2014.
- 79. Kim, D.H., Shin, H.J., Lee, H., Jeong, C.K., Park, H., Hwang, G.-T., Lee, H.-Y., Joe, D.J., Han, J.H., Lee, S.H., Kim, J., Joung, B., Lee, K.J., In Vivo self-powered wireless transmission using biocompatible flexible energy harvesters, Adv. Funct. Mater., 27, 25, 1700341, 2017.
- 80. Feng, H., Zhao, C., Tan, P., Liu, R., Chen, X., Li, Z., Nanogenerator for biomedical applications, Adv. Healthc. Mater., 7, 10, 1701298, 2018.
- 81. Shi, B., Li, Z., Fan, Y., Implantable energy-harvesting devices, Adv. Mater., 30, 44, 1801511, 2018.
- 82. Li, Z., Zhu, G., Yang, R., Wang, A.C., Wang, Z.L., Muscle-driven in vivo nanogenerator, Adv. Mater., 22, 23, 2534–2537, 2010.
- 83. Buzsaki, G., Anastassiou, C.A., Koch, C., The origin of extracellular fields and currents — EEG, ECoG, LFP and spikes, Nat. Rev. Neurosci., 13, 6, 407– 420, 2012.
- 84. Lotte, F., Bougrain, L., Clerc, M., Electroencephalography (EEG)-based brain–computer interfaces, Wiley Encyclopedia of Electrical and Electronics Engineering, Wiley, 2015.
- 85. Kubler, A., Nijboer, F., Mellinger, J., Vaughan, T.M., Pawelzik, H., Schalk, G., McFarland, D.J., Birbaumer, N., Wolpaw, J.R., A review of organic and inorganic biomaterials for neural interfaces, Neurology, 64, 1775, 2005. Fattahi, P., Yang, G., Kim, G., Abidian, M.R., Adv. Mater., 26, 12, 1846–1885, 2014.
- 86. Yang, T., Hakimian, S., Schwartz, T.H., Intraoperative ElectroCorticoGraphy (ECog): Indications, techniques, and utility in epilepsy surgery. Epileptic Disord., Wiley online library, 16, 3, 271–279, 2014.
- 87. Shin, G., Gomez, A.M., Al-Hasani, R., Jeong, Y.R., Kim, J., Xie, Z., Banks, A., Lee, S.M., Han, S.Y., Yoo, C.J., Lee, J.L., Lee, S.H., Kurniawan, J., Tureb, J., Guo, Z., Yoon, J., Park, S., II, Bang, S.Y., Nam, Y., Walicki, M.C., Samineni, V.K., Mickle, A.D., Lee, K., Heo, S.Y., McCall, J.G., Pan, T., Wang, L., Feng, X., Kim, T., II, Kim, J.K., Li, Y., Huang, Y., Gereau, R.W., Ha, J.S., Bruchas, M.R., Rogers, J.A., Flexible near-field wireless optoelectronics as subdermal implants for broad applications in optogenetics, Neuron, 93, 3, 509–521.e3, 2017.
- 88. Hong, G., Yang, X., Zhou, T., Lieber, C.M., Mesh electronics: A new paradigm for tissue-like brain probes, Curr. Opin. Neurobiol., 50, 33–41, 2017.
- 89. Jia, Y., Khan, W., Lee, B., Fan, B., Madi, F., Weber, A., Li, W., Ghovanloo, M., Wireless opto-electro neural interface for experiments with small freely behaving animals, J. Neural Eng., 15, 4, 046032, 2018.
- 90. Lee, S. and Lee, C., Toward advanced neural interfaces for the peripheral nervous system (PNS) and their future applications, Curr. Opin. Biomed. Eng., 6, 130–137, 2018.
- 91. Wang, J., Thow, X.Y., Wang, H., Lee, S., Voges, K., Thakor, N.V., Yen, S.C., Lee, C., Intelligence toward future implanted body sensor networks, Adv. Healthc. Mater., 7, 5, 1700987, 2018.
- 92. Clements, I.P., Mukhatyar, V.J., Srinivasan, A., Bentley, J.T., Andreasen, D.S., Bellamkonda, R.V., Regenerative scaffold electrodes for peripheral nerve interfacing. IEEE Trans. Neural Syst. Rehabil. Eng., 21, 4, 554–566, 2013.
- 93. Delgado-Martinez, I., Righi, M., Santos, D., Cutrone, A., Bossi, S., D’Amico, S., Del Valle, J., Micera, S., Navarro, X., Fascicular nerve stimulation and recording using a novel double-aisle regenerative electrode, Neural Eng., J., 14, 4, 046003, 2017.
- 94. Rossini, P.M., Micera, S., Benvenuto, A., Carpaneto, J., Cavallo, G., Citi, L., Cipriani, C., Denaro, L., Denaro, V., Pino, G.D., Ferreri, F., Guglielmelli, E., Hoffmann, K.P., Raspopovic, S., Rigosa, J., Rossini, L., Tombini, M., Dario, P., Erratum to implantable neurotechnologies: Bidirectional neural interfaces—Applications and VLSI circuit implementations, Clin. Neurophysiol., 121, 777, 2010.
- 95. Bri, D., Garcia, M., Lloret, J., Dini, P., Real deployments of wireless sensor networks, in: Proceedings of the 3rd International Conference on Sensor Technologies and Applications (SENSORCOMM ‘09), Athens, Greece, pp. 415–423, June 2009.
- 96. Sahadevaiah, K. and Prasad Reddy, P.V.G.D., Impact of security attacks on a new security protocol for mobile ad hoc networks. Network protocols and algorithms, Network Protoc. Algorithms, 3, 4, 122–140, 2011.
- 97. Alrajeh, N.A., Khan, S., Lloret, J., Loo, J., Artificial neural network based detection of energy exhaustion attacks in wireless sensor networks capable of energy harvesting, Ad Hoc Sens. Wirel. Netw., 2013, 1–25, 2013.
- 98. Sisodia, M.S. and Raghuwanshi, V., Anomaly base network intrusion detection by using random decision tree and random projection a fast network intrusion detection technique. Network Protoc. Algorithms, 3, 4, 93–107, 2011.
- 99. Lim, T.H., Detecting Anomalies in Wireless Sensor Networks [Qualifying Dissertation], Department of Computer Science, University of York, 2010.
- 100. Kim, J., Bentley, P., Wallenta, C., Ahmed, M., Hailes, S., Danger is ubiquitous: Detecting malicious activities in sensor networks using the dendritic cell algorithm, in: Artificial Immune Systems, Lecture Notes in Computer Science, vol. 4163, pp. 390–403, Springer, Berlin, Germany, 2006.
- 101. Drozda, M., Schaust, S., Szczerbicka, H., AIS for misbehavior detection in wireless sensor networks: Performance and design principles, in: Proceedings of the IEEE Congress on Evolutionary Computation (CEC ‘07), pp. 3719–3726, September 2007.
- 102. Alrajeh, N., Khan, S., Lloret, J., Loo, J., Artificial neural network based detection of energy exhaustion attacks in wireless sensor networks capable of energy harvesting. Ad Hoc Sens. Wirel. Netw., 2013, 1–25, 2013.
- 103. Mukherjee, P. and Sen, S., Using learned data patterns to detect malicious nodes in sensor networks, in: Distributed Computing and Networking, Lecture Notes in Computer Science, vol. 4904, pp. 339–344, Springer, Berlin, Germany, 2008.
- 104. Li, Y.Y. and Parker, L.E., Intruder detection using a wireless sensor network with an intelligent mobile robot response, in: Proceedings of the IEEE Southeast Conference, pp. 37–42, April 2008.
- 105. Abdullah, B., Abd-alghafar, I., Salama, G., II, Abd-alhafez, A., Performance evaluation of a genetic algorithm based approach to network intrusion detection system, in: Proceedings of the International Conference on Aerospace Sciences and Aviation Technology, Military Technical College, Cairo, Egypt, 2009.
- 106. Khanna, R., Liu, H., Chen, H.-H., Reduced complexity intrusion detection in sensor networks using genetic algorithm, in: Proceedings of the IEEE International Conference on Communications (ICC ‘09), pp. 1–5, June 2009.
- 107. Lusted, L.B., Medical progress – medical electronics. N. Engl. J. Med., 252, 580–5, 1955.
- 108. Ledley, R.S. and Lusted, L.B., Reasoning foundations of medical diagnosis. Science, 130, 9–21, 1959.
- 109. Steimann, F., On the use and usefulness of fuzzy sets in medical AI. Artif. Intell. Med., 21, 131–7, 2001.
- 110. Gunn, A.A., The diagnosis of acute abdominal pain with computer analysis. J. R. Coll. Surg. Edinb., 21, 170–2, 1976.
- 111. Hopfield, J.J., Neural networks and physical systems with emergent collective computational abilities. Proc. Natl. Acad. Sci. U.S.A., 79, 2554–8, 1982.
- 112. Boon, M.E. and Kok, L.P., Neural network processing can provide means to catch errors that slip through human screening of pap smears. Diagn. Cytopathol., 9, 411–6, 1993.
- 113. Downs, J., Harrison, R.F., Kennedy, R.L., Cross, S.S., Application of the fuzzy ARTMAP neural network model to medical pattern classification tasks. Artif. Intell. Med., 8, 403–28, 1996.
- 114. Ashizawa, K., Ishida, T., Mac Mahon, H., Vyborny, C.J., Katsuragawa, S., Doi, K., Artificial neural networks in chest radiography: Application to the differential diagnosis of interstitial lung disease. Acad. Radiol., 6, 2–9, 1999.
- 115. Tailor, A., Jurkovic, D., Bourne, T.H., Collins, W.P., Campbell, S., Sonographic prediction of malignancy in adnexal masses using an artificial neural network. Br. J. Obstet. Gynaecol., 106, 21–30, 1999.
- 116. Lucht, R., Delorme, S., Brix, G., Neural network-based segmentation of dynamic MR mammographic images. Magn. Reson. Imaging, 20, 147–54, 2002.
- 117. Burke, H.B., Hoang, A., Iglehart, J.D., Marks, J.R., Predicting response to adjuvant and radiation therapy in patients with early stage breast carcinoma. Cancer, 82, 874–7, 1998.
- 118. Dybowski, R., Weler, P., Chang, R., Gant, V., Prediction of outcome in critically ill patients using artificial neural network synthesised by genetic algorithm. Lancet, 347, 1146–50, 1996.
- 119. Han, M., Snow, P.B., Epstein, J., II, Chan, T.Y., Jones, K.A., Walsh, P.C. et al., A neural network predicts progression for men with Gleason score 3+4 versus 4+3 tumors after radical prostatectomy. Urology, 56, 994–9, 2000.
- 120. Zadeh, L.A., Fuzzy sets. Inf. Control, 8, 338–53, 1965.
- 121. Halm, U., Rohde, N., Klapdor, R., Reith, H.B., Thiede, A., Etzrodt, G. et al., Improved sensitivity of fuzzy logic based tumor marker profiles for diagnosis of pancreatic carcinoma versus benign pancreatic disease. Anticancer Res., 20, 4957–60, 2000.
- 122. Verma, B. and Zakos, J., A computer-aided diagnosis system for digital mammograms based on fuzzy-neural and feature extraction techniques. IEEE Trans. Biomed. Eng., 5, 46–54, 2001.
- 123. Sztandera, L.M., Goodenday, L.S., Cios, K.J., A neuro-fuzzy algorithm for diagnosis of coronary artery stenosis. Comput. Biol. Med., 26, 97–111, 1996.
- 124. Behloul, F., Lelieveldt, B.P., Boudraa, A., Janier, M.F., Revel, D., Reiber, J.H., Neurofuzzy systems for computer aided myocardial viability assessment. IEEE Trans. Med. Imaging, 20, 1302–13, 2001.
- 125. Bellman, R., An Introduction to Artificial Intelligence: Can Computers Think?, Thomson Course Technology, 1978.
- 126. Deo, R.C., Machine learning in medicine. Circulation, 132, 20, 1920–1930, 2015. [PubMed: 26572668].
- 127. Sutton, R.S. and Barto, A.G., Reinforcement learning: An introduction. Vol. 1, MIT Press, Cambridge, 1998.
- 128. Miller, R.A., Pople, H.E.J., Myers, J.D., Internist-I, an experimental computer-based diagnostic consultant for general internal medicine. N. Engl. J. Med., 307, 8, 468–476, NEJM group, 1982. [PubMed: 7048091].
- 129. Smith, R.O., The emergence and emergency of assistive technology outcomes research methodology. Assistive Technol. Outcomes Benefits, 10, 1, 19–37, 2016.
- 130. Talbot, T.B., Sagae, K., John, B., Rizzo, A.A., Sorting out the virtual patient: How to exploit artificial intelligence, game technology and sound educational practices to create engaging role-playing simulations. Int. J. Gaming Comput.-Mediat. Simul., 4, 3, 1–19, 2012. http://dx.doi.org/10.4018/jgcms.2012070101.
- 131. van den Heuvel, R.J., Lexis, M.A., Gelderblom, G.J., Jansens, R.M., de Witte, L.P., Robots and ICT to support play in children with severe physical disabilities: A systematic review. Disabil. Rehabil. Assist. Technol., 11, 103–116, 2016.
- 132. Celi, L.A., Moseley, E., Moses, C., Ryan, P., Somai, M., Stone, D. et al., From pharmacovigilance to clinical care optimization. Big Data, 2, 134–41, 2014.
- 133. Helpman, E. and Trajtenberg, M., Diffusion of general purpose technologies. NBER Work. Pap. Ser., Working paper series 5773, 1996.
- 134. Trajtenberg, M., AI as the next GPT: A Political-Economy Perspective, NBER Work. Pap. Ser., w24245, 2018.
- 135. Johnson, A.E., Pollard, T.J., Mark, R.G., Reproducibility in critical care: A mortality prediction case study. Machine Learning for Healthcare Conference, November 2017.
- 136. Gibson, D.G., Ochieng, B., Kagucia, E.W. et al., Mobile phone-delivered reminders and incentives to improve childhood immunisation coverage and timeliness in Kenya (M-SIMU): A cluster randomized controlled trial. Lancet Glob. Health, 5, e428–38, 2017.
- 137. Stockwell, M.S., Kharbanda, E.O., Martinez, R.A. et al., Effect of a text messaging intervention on influenza vaccination in an urban, low-income pediatric and adolescent population: A randomized controlled trial. JAMA, 307, 1702–8, 2012.
- 138. Haskew, J., Rø, G., Saito, K. et al., Implementation of a cloud-based electronic medical record for maternal and child health in rural Kenya. Int. J. Med. Inform., 84, 349–54, 2015.
- 139. Haskew, J., Ro, G., Turner, K. et al., Implementation of a cloud-based electronic medical record to reduce gaps in the HIV treatment continuum in Rural Kenya. PloS One, 10, e0135361, 2015.
- 140. Piette, J.D., Mendoza-Avelares, M.O., Ganser, M. et al., A preliminary study of a cloud-computing model for chronic illness selfcare support in an underdeveloped country. Am. J. Prev. Med., 40, 629–32, 2011.
- 141. Utermohlen, K., Four robotic process automation (RPA) applications in the healthcare industry. Medium, 2018.
- 142. UserTesting, Healthcare Chatbot Apps are on the Rise but the Overall Customer Experience (cx) Falls Short According to a UserTesting Report, UserTesting, San Francisco, 2019.
- 143. Lohr, S., IBM is counting on its bet on Watson, and paying big money for it, New York Times, 17, 10, 2016.
- 144. Otake, T., IBM big data used for rapid diagnosis of rare leukemia case in Japan, The Japan Times, 2016.
- 145. Graham, J., Artificial intelligence, machine learning, and the FDA, 2016.
- 146. Barber, F., Botti, V.J., Koehler, J., AI: Past, present and future. Upgrade the European Online Magazine for the IT Professional, 3, 5.
- 147. Savadjiev, P., Chong, J., Dohan, A., Vakalopoulou, M., Reinhold, C., Paragios, N., Gallix, B., Demystification of AI-driven medical image interpretation: Past, present and future. Eur. Radiol., 29, 3, 1616–1624, 2019.
Note
- *Corresponding author: [email protected]