
"Today's design and construction environment is extraordinarily complex. Clients have to make an increasing number of decisions that have lasting impact on both their operations and communities. For architects to contribute value to these clients, we have to seize the opportunity to move beyond intuition and to provide rigorously developed evidence about predictive relationships between design and human response. Our clients will benefit most from the design process if we inform decisions with credible (scientific) research." | ||
| --—Gordon Chong, FAIA, Project Director, 2005 Latrobe Fellowship | ||
This book is about a transformation occurring in the architectural profession. The previous chapters exemplify how developing and applying evidence can enhance creative design, particularly in the realms of building and environmental science. Most architects, by virtue of traditional architectural education and practice, can relate to the extraordinary engineering and formal aspects of this achievement.
The future profession we envision will be equally effective in creating architecture that enhances human performance. As specifically illustrated in some of the work of the experts highlighted in Chapters 2 through 4, significant advances have been made in linking design and human response. However, as a whole profession, we are at an early point in this journey.
Biennially, the American Institute of Architects (AIA) College of Fellows awards a grant, named for architect Benjamin Henry Latrobe, for research leading to significant advances in the architecture profession. The 2005 Latrobe Fellowship was awarded to Chong Partners Architecture (now Stantec Architecture), Kaiser Permanente, and the University of California, Berkeley, to explore the use of evidence from the social and physiological sciences to better understand human response to physical enviornments, and thereby make better design decisions that create places for better healing, learning, and work collaboration and productivity.
The research focused specifically on health-care environments and the question of whether design can aid healing (reduced "time to heal" and medical errors, in turn, increase hospital financial performance). Credible evidence of design impacts on healing and errors does exist; but so do assertions based on very weak indicators. The Latrobe research sought a model for creating evidence that would be reliably strong, meaningful in terms a client would value, and inspirational.
As with many explorations relatively early in a transformation, the 2005 Latrobe followed a different course than what was initially expected. But it resulted in lessons of value for all design practitioners. Some are applicable today and others point toward a future with a much greater degree of predictability for design outcomes. These will be discussed in two categories: (1) the Process Model and Methodologies; and (2) the Literature and Experimental Findings.
THE 2005 LATROBE HYPOTHESIS:
CREDIBLE, APPLICABLE "EVIDENCE" OF RELATIONSHIPS BETWEEN DESIGN AND CLIENT ORGANIZATIONAL PERFORMANCE WILL RESULT FROM (1) A COLLABORATIVE APPROACH THAT UNITES THE PERSPECTIVES, SKILLS, AND RESOURCES OF THE ARCHITECTURAL FIRM, UNIVERSITY RESEARCH COMMUNITY, AND CLIENT; AND (2) USE OF BOTH SCIENTIFIC RESEARCH METHODS AND INDUCTIVE REASONING ARE CRITICAL TO THE PROCESS.
The Latrobe research team posed and examined this hypothesis using a research model with three characteristics:
Collaboration among a practicing architectural firm, a university research community, and a leading health-care provider to seek the best ways to utilize the skills and knowledge of all three in a trans-disciplinary framework.
Use of behavioral sciences, biomedical and neuroscience methodologies, as well as inductive reasoning
Application of metrics to measure human responses to various design conditions and to evaluate organization performance impacts
The research was intended to assess the usefulness of this three-part model for future design evidence production, as well as to compile and create knowledge for design application in the short term.
The strength of much of the work discussed in Chapters 2 through 5 of this book derives from teams with diverse skills and experience. Understanding the client's needs, the design process, and research quality standards are all needed to develop evidence for design that is both scientifically defensible and applicable. Therefore, experts in this book advocate that architects would benefit from engaging people from various disciplines in the evidence-building process.
The Latrobe team tried to demonstrate the validity of this theory. From experience in design practice, research, and education, the 2005 Latrobe research team agreed at the outset that architects, academic researchers, and clients approach knowledge production and management differently. Architects have valuable experience, technical knowledge, and creative skills, but often rely more on intuition than evidence backed by rigorous research. University researchers understand scientific protocols but work in isolation from the people who best understand the questions of most value to answer. Therefore, many from this community pursue topics of scholarly interest that have limited applicability. And then there are the in-house facilities and real estate professionals. They might believe that design has the power to support their core business goals but they lack access to the "evidence" they need to make credible business cases, backed by relevant financial and other performance metrics. Ultimately, not being able to sell the investment in an innovative design, they end up delivering cost-conscious environments that are suboptimal in terms of their influence on human outcome.
The Latrobe team wanted to examine an approach to creating evidence for design that was more powerful than what each constituent might be able to do alone. An inspiration came from the research framework known as Mode 2 Knowledge Production (Gibbons et al.). The principles of Mode 2 are useful guidelines for any design practitioner with an interest in evidence for design. Unlike the more traditional Mode 1 research, typical of work developed solely in academia, Mode 2 engages the skills and perspectives of people, such as architects and their clients, who understand how the research will be practically applied and how success will be evaluated.
Consider these five Mode 2 characteristics. They provide a platform for designers to meaningfully develop and interpret design research.
It is generated in the context of application. It arises from the very work of problem resolution, e.g., a design innovation intended to promote a human performance outcome.
It is trans-disciplinary. A range of methods, e.g., design charrette and behavioral survey, is used with tools and perspectives coming together often in novel forms to solve a specific problem.
It is produced across knowledge organizations, e.g., design firm, health-care provider and research institute, and in a variety of settings.
It is reflexive, in that there is conversation between the researchers—scientists and designers—and the subjects—client organizations. The problem-resolution environment influences the topic, the research design, and the end uses.
It must accommodate multiple definitions of quality because there are many players and a lack of strict disciplinary criteria with which scientific peers can evaluate. (For example, the designer and client may judge if the research has been sufficient to influence the desired results.)
Many designers believe that scientific research and design process are incompatible. Science is not trusted because it appears to have no room for artistic inspiration. Evidence created by scientific research is feared to be overly prescriptive, limiting the designer's range of expression. One could argue that this is an erroneous view and that creativity plays a major role in shaping scientific research design. However, when Mode 2 knowledge development is used in the context of evidence-based design, the debate becomes moot because the designer is a participant and the design process integral to shaping the intent and outcome. For the Latrobe, designers worked side by side with neuroscientists, social scientists, and the client to enhance the usefulness of the research outcomes.

Behavioral sciences have been at the heart of environmental design research for many years. They continue to be powerful in revealing and communicating linkages between design attributes and human response. Although social science methods require rigor to be valid, they can be fairly readily adapted to the looser design inquiry process within project schedules and budgets.
The use of physiological responses to environmental stimuli is more recent and more complex. Neuro-architecture, for example, is early in its development. Nevertheless, the understanding of how the body responds to specific aspects of place promises new levels of capability in affecting human performance in the realms of health and cognitive performance. We will no longer have to rely on self-assessment of what causes productivity but actually witness brain functionality in different spaces, as measured by very specific causal elements.
The 2005 Latrobe sought to introduce an element of physiological measurement, in order to push forward this new way of assessing design effectiveness. It did so by seeking both medical data (in a data mining exercise at KP) and stress measures (in an experiment conducted at several university labs).
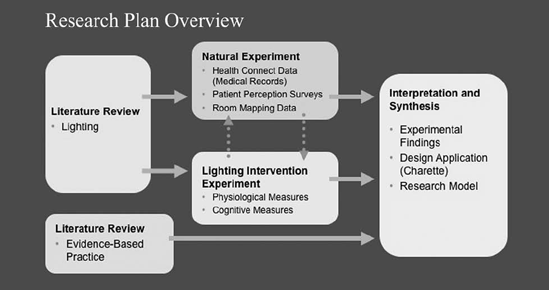
The research plan comprised four major tracks. Following a literature search, two types of experiments were conducted, based on what team members believed would be the most productive methodology. Although this dual track diverged from the intended "trans-disciplinary" approach, it had potential to investigate one issue from two perspectives and then discover if the two methods reinforced each other. The following illustrates the four components of this research effort:
Problem Definition and Research Plan
Team building/Establishing goals
Engaging stakeholders and experts
Preliminary literature search
Lighting and health
Color and health
Evidence-based practice
Refining pilot study topic(s)
Research plan development
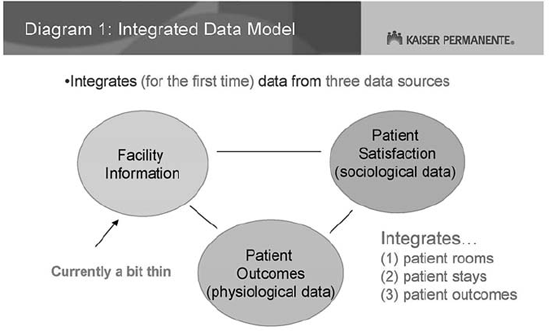
The Natural Experiment (The Kaiser Permanente (KP) Integrated Data Model—IDM), Principal Investigator: Robert Mangel, PhD. (See credits at end of this chapter for the many contributors from KP.)
Many organizations collect extensive data to monitor their own performance effectiveness. The concept of the IDM was to link physiological and opinion data, routinely collected within KP's medical records and patient surveys, with design attributes of the rooms occupied by the corresponding patients. Data mining would then support queries such as "Do patients in rooms with northern daylight exposure heal or feel differently from those with southern light?"
The large volume of data would create very strong, continually refreshing evidence without being intrusive to staff or patients. Large samples are one way to diminish the impacts of naturally occurring variations that are difficult to control in complex environments, e.g., hospitals. In addition, large-scale studies have other appealing aspects for corporate decision-making, in that executives with decision authority are often accustomed to benchmarking and other large survey-type research. In addition to analyzing existing physical conditions, the IDM system could be used to measure the effects of direct design interventions, e.g., room modifications, hypothesized based on other research discovered through literature search or even based on intuition and experience.
Envisioned was an integrated database with attributes of 30 hospitals (totaling over 60 million square feet) and perhaps 100,000 patient stays cumulative over time. At the time of completion of the Latrobe, the IDM was designed and being implemented. Early pilots supported the notion of its power but there were no design findings to be reported with high confidence.
The Laboratory Experiment, Principal Investigator: Eve Edelstein, PhD. (See credits at end of this chapter for the full research team.)
This approach was based on using rigorously controlled experimental (lab) conditions and multiple measures to enhance the strength of evidence. Physiological and cognitive responses to specific light qualities were analyzed and interpreted in the context of an extensive literature base. Although by definition, lab research is Mode 1, this experiment was conceived jointly with the trans-disciplinary team to address some critically important design issues; and it was complemented by field measurements and design charrettes, thereby relating it more closely to Mode 2 applications.
The Model, Principal Investigator: W. Mike Martin, PhD., FAIA (See credits at the end of this chapter for the full research team.)
The research approach itself was observed and analyzed as it unfolded to assess its value for future design research.
Integrating active medical records data with design attributes captured in an equally "active" CAFM system is a very powerful method for future health-care EBD research. (Parallel opportunities to mine organizational performance data exist in other types of institutions.)
Physiological data, such as heart rate variability and EEG brain waves, can be very compelling evidence for design, as it has been proven to indicate health risk, health status, and cognitive function.
One concern about laboratory experimentation as a method used in EBD is that it does not directly assess real life design applications. Nevertheless, the use of scientific method, including controlled research design and statistical analysis of results to substantiate the reliability and validity, increases strength of evidence. Combining lab findings with design intuition and field interventions can create solid evidence.
Each research approach used to build evidence that informs design has its limitations. Evidence is perhaps best if looked at from multiple perspectives (opinion surveys, observation of behavioral performance, laboratory experiments, or in-field measuring of environmental conditions), and subject to various measures (organizational, economic, psychological, social, and physiological).
Literature searches about evidence-based practice and lighting (the focal topic of the Latrobe pilots) discovered useful information that practitioners can use today. The laboratory experiments also resulted in lessons learned to inform design decision-making.
The team researched precedents for evidence-based practice in Design, Medicine, Management, and Education. (This effort was led by Robert Brandt, Steven Doctors, and Eve Edelstein.) A few common guiding principles emerged that might be useful to design practitioners who are establishing their own approaches or trying to critically assess those of others.
There are a variety of types of useful and credible evidence.
How "strong" the evidence is, i.e., how powerful it is in terms of predicting an outcome or describing a relationship between two factors (such as "view" and "healing"), will depend on the methodology used to create the evidence.
The basic rules of scientific research do apply. Evidence should be "valid," i.e., it should address the topic it is intended to address (and not be a reflection of another superfluous condition), and it should be "repeatable," i.e., we can feel fairly sure the results will recur. These seem obvious, but how often do we jump to a solution based on a single observation rather than a body of knowledge? As designers, we want answers. But are they the right answers? Was it the "daylight" or the "view" that caused a particular patient response? If we don't know, how can we decide about the size, placement, and orientation of windows beyond merely what feels right?
Taken together, greater control of potentially superfluous factors, consistency of results across subject groups, and a fairly tight range of responses among research subjects increase the value of research data as a predictor.
Careful experimental design, including randomization and control, increases the strength of research results, as do large datasets and systemized methodologies.
There is value in having commonly accepted standards for attributing value to knowledge intended to be applied as evidence. (We embrace "evidence-based design," but does that mean the same thing to all of us? Not currently.)
Evidence-based practice does not necessarily remove the soul from practice. The practitioner's judgment and values, informed by experience, are central.
Context must always be considered.
A key consideration in evidence-based practice is communication. We must demand to know enough about the source, the context in which it was developed, and methods used to create evidence, to make a responsible decision about how seriously to trust that evidence and to decide when it's relevant to apply it.
The following is extracted from the literature review conducted by Eve Edelstein, PhD, and contained in the 2005 Latrobe Research Report.
Many behavioral and physiological responses are now associated in the literature with exposure to electrical lighting, daylight, and solar orientation. The field has progressed through multiple generations of study, Which include the investigation of endocrine changes related to electrical light exposures, such as the role of melatonin in sleep and wake cycles.
Human studies have disclosed that cardiac rhythms, stress, endocrines, hormones, growth and aging, developmental, cognitive, and emotional responses demonstrate circadian rhythms in normal individuals. The evidence base reveals diseases and disorders associated with disruption of circadian or circannual light conditions. For example, hypertension may be related to the disruption of normal diurnal conditions and cancer risk may be associated with light-induced disruption of melatonin production (which is implicated in the control of cancer growth). Seasonal Affective Disorder is now an accepted consequence of seasonal lighting and climactic changes, and electrical light therapies are being actively investigated.
The categories below represent a partial list of human responses to light.
Stress, modulation of cortisol/stress hormones
Heart disease and hypertension
Melatonin responses
Sleep/activity/feeding cycles
Cancer
Basal metabolic rate, protein synthesis, and thyroid responses
Growth
Aging responses
Hormone function
Obstetric
Neonatal responses
Ophthalmic development and health
Hyperbilirubinemia and kernicterus
Long-term visual function in NICU graduates
Gastro-intestinal conditions
Diabetes
Neural immune responses
Inflammation and autoimmune disorders
Brain development and function
Ataxia, neuropathy
Concentration
Alertness
Attention deficit disorder
Working memory
Psychologic and psychiatric conditions
Decreased memory, dementia
Depression, emotional labiality
Seasonal Affective Disorders
Pain
Perception and self-report of pain and pain management
Medication rates relative to lighting dosage and length of stay
Circadian cycles can be modulated by a variety of external cues, but light is the primary variable that aligns (or entrains) humans to diurnal, nocturnal, and seasonal rhythms. In 2001, a new class of cells Was discovered in the retina of the eye, thought to be "circadian" receptors that sense slow changes in light levels, rather than receptors for vision. This discovery renewed research to explore the spectrum, intensity, and duration of light that influence biological responses.
Numerous studies have led to the development of "dose response curves" to electrical light that reveal peak sensitivity in the blue wavelength (between 420 and 470 nm) for modulations of melatonin suppression that regulates sleepiness. Bright white light has also been demonstrated to be effective in modulating mood, sleep, and activity cycles (Ancoli-Israel et al., 2003).
The range of spectra that influence the multiple circadian systems is yet to be fully explored. Although research has focused on short wavelengths in the blue range, a broader range of spectra is also associated with biological responses (Revell et al., 2006). Testing of red light has been uncommon, and many researchers have assumed that there is little to no effect of red light on the neuroendocrine or circadian systems. However, Hanifin and colleagues (2005) found that normal healthy humans exposed to 630 nm and 700 nm elicited small reductions of plasma melatonin levels. These findings are consistent with other studies that reveal the influence of a long wavelength light on cardiac responses (Schafter and Kratky, 2006).
The laboratory experiment used rigorously designed and controlled conditions to demonstrate specific changes related to alterations of the environment. Measurement methods most likely to yield statistically valid results were selected based on the literature review. Statistical significance was achieved by minimizing the complexity of the test environment and by testing the influence of one environmental change at a time.
The laboratory experiment explored how architecture might influence human exposure to light within built settings, and how varied light levels and spectra might influence health outcomes. Medical research acknowledges that chronic stress is a major contributor to heart attack, cancer, and diabetes. Further, we are able to alter lighting and to measure heart rate variability and EEG (key indicators of stress); thus determining linkages between lighting and health outcomes.
The Latrobe experiment showed that heart rate activation increased and variability decreased during brief exposure to bright white light (with a peak in the blue spectrum) during exposure. These results are consistent with melatonin studies using longer exposures at night. Yet more interesting were the results that showed that heart rate responses were highly significantly different in red light conditions from those in white light; with the red light associated with situationally appropriate cardiac activation and relaxation during cognitive tasks.
Following the experiment, a team of designers and client representatives considered the findings and interpreted how they might apply to design. This step is inductive, and the team did not intend to imply that the design ideas have been rigorously tested and validated. However, the interpretive process illuminates how the design process can come together with scientific evidence to strengthen the creative process.
Several design charettes were held to discuss the potential impact of introducing biologically relevant light levels on architecture and design. How did the design team interpret the experimental findings and related survey of the literature?
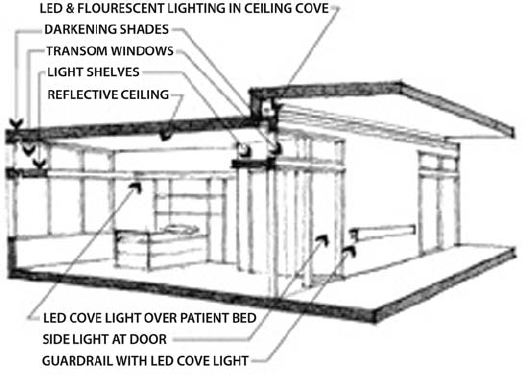
The need for light is well known but circadian systems also require periods of darkness. In many current hospitals, light intrusion into patient rooms from outside the building, as well as from corridors and other proximate interior spaces, is often at levels sufficient to disrupt the patient's circadian rhythms.
Design Interpretation
Patient rooms must have the ability to be darkened, including an ability to control light intrusion from both outside and inside the building.
Accessible controls should provide patients with the ability to adjust light for their individual needs. A single-touch, programmable control for medical staff to immediately establish optimal lighting for assessment and procedures should be provided at bedside and/or at clinical stations.
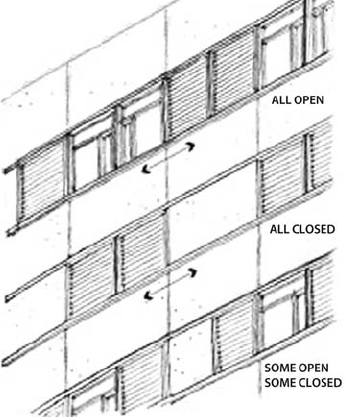
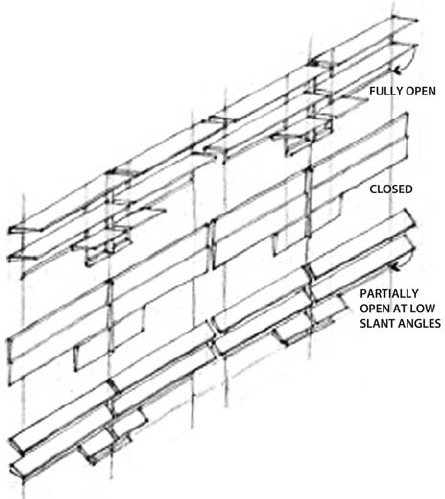
Achieving optimal light level starts outside the building, with external shading and shielding devices. A kinetic skin that adapts to seasonal and diurnal light changes (but has manual overrides) may help balance needs for circadian light and darkness, view and glare control.
Shades should be installed to effectively seal out light around the window perimeter.
Low-intensity lighting on the corridor side of the patient room walls may reinforce pathways for safety while not limiting light pollution into patient rooms.
Natural daylight can be considered the "gold standard" and it comprises different frequencies, intensities, and dynamic patterns of light exposure that are related to measurable differences in biological responses. Constant exposure to a single frequency and level of light is not ideal for normal circadian patterns. Daylight and electrical lighting that emulates natural diurnal, nocturnal, and seasonal cycles is most likely to support circadian needs and health.
Design Interpretation
Brightness and frequency of light should vary throughout the day. The objective is to provide the appropriate cycle frequency of light, including light in the range of spectra and intensities—blue and bright white spectra, known to influence melatonin-related sleep/wake cycles, and red spectrum, which influences heart rate variability.
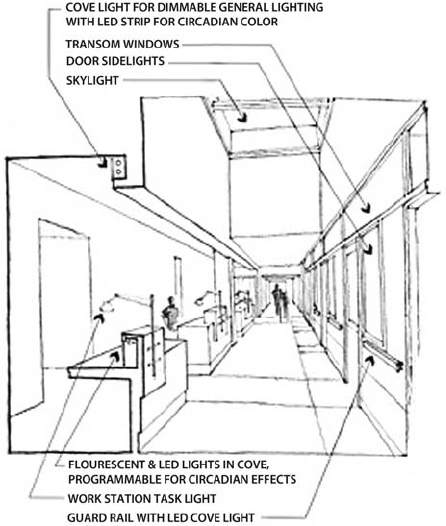
Building core and shell design should allow for controlled daylight penetration to the central nursing stations or team work areas (often not currently provided in interior areas of large-footprint buildings).
Atria and light wells might, but do not necessarily, provide sufficient circadian light to interior areas. Orientation, floor level, and atrium proportions should be modeled for circadian light frequency, as well as intensity. (The two do not always correspond.)
Light shelves may be used to introduce daylight to corridors where "borrowed light" to the distributed nursing areas is often blocked by doors, window coverings, and bed drapes.
Staff should have access to spaces for both darkness and light. There should be a break room with daylight, as well as a separate on-call room to serve different circadian needs, especially for transitioning shift workers.
For areas where daylight is not feasible or practical (such as imaging rooms), [there should be] controlled electrical lighting that can be varied according to user, function, frequency, intensity, and distribution to provide useful circadian stimulation.
For night shift and swing shift workers, daytime patterns of light frequency variation should be recreated and provided to the extent feasible while still supporting patient needs for darkness and staff needs for visual acuity, safety, and security. The use of white and blue frequency light augmented by task and safety lighting may support staff circadian sleep/wake patterns. Red light in corridors could be explored as a means to support night time monitoring while minimizing circadian sleep/wake patterns in patients. White lighting at clinical stations would provide for task-related visual acuity. Individual controls at staff stations are essential.
Localized "light showers" (brief exposure to light that stimulates the melatonin systems) at distributed desks may provide for needed circadian activation.
Low level ambient light should be complemented by task lighting at work centers for visual acuity. Bright light should be screened so as not to penetrate into patient rooms.
Lighting needs vary by individual medical condition, visual acuity, preference, and culture. An individual's history of light exposure (over several hours, days, weeks) influences his or her need for circadian light. Swing and especially night shift workers may suffer from stress responses due to misalignment of their sleep/wake cycles and natural daylight and darkness.
Design Interpretation
Lighting controls are as important as lighting. Patient and family are likely to make preferred adjustments, but they may not know what light is healthiest. The ideal system would combine computerized control to provide desirable circadian light (that the patient or staff may not choose) and overrides to adapt to preferences.
Patient controls must be accessible and easy to use, and should allow control of electric light as well as window coverings.
Cultural preferences may have a great influence on color choices. Patient control of color through LED lighting may provide a sense of control and ability to easily adapt the environment as the needs and preferences of occupants change.
Special lighting needs should be considered when setting such levels. For example, elder patients are more likely to need greater light levels, but may be more disturbed by glare and reflection.
The 2005 Latrobe Fellowship was sponsored by the American Institute of Architects College of Fellows.
Gordon H. Chong, FAIA, Chong Partners Architecture[14]
Robert M. Brandt, AIA, Chong Partners Architecture*
Galen Cranz, PhD, University of California, Berkeley
Barbara P.Denton, Assoc. AIA, Kaiser Permanente (KP)*
Steven I. Doctors, PhD Candidate, University of California, Berkeley
Eve A.Edelstein, MArch, PhD, Consultant to Chong Partners Architecture*
Robert S. Mangel, PhD, Kaiser Permanente (KP)
W. Mike Martin, PhD, FAIA, University of California, Berkeley*
Chong Partners Architecture (now Stantec Architecture)
THE LABORATORY EXPERIMENT RESEARCH TEAM
Eve A. Edelstein, Ph.D Principal Investigator
Division of Biological Sciences, University of California, San Diego Academy of Neuroscience for Architecture
Robert J. Ellis, John J.Sollers III, Ph.D., Julian F. Thayer, Ph.D.
Department of Psychology, Ohio State University, Columbus
Ruey-Song Huang, Ph.D., Tzyy-Ping Jung, Ph.D., Scott Makeig, Ph.D.
The Swartz Center for Computational Neuroscience, University of California, San Diego
Robert Brandt, AIA Team Leader for Chong Partners Architecture
We acknowledge the generous contributions of time, expertise, equipment, and laboratory resources by our advisors and contributors.
CHONG PARTNERS ARCHITECTURE
Katherine Anderson
Teresa Au
Cathy Barrett
Larry Bongort
Edward Dean
Jeff Farley
Bret Harper
Roland Lau
John Sealander
Giovanni Succi
Chris Tymoff
UNIVERSITY OF CALIFORNIA, BERKELEY
Gabriel Arboleda, Arch Ph.D. student
Professor Cris Benton, Architecture Department
Professor Harrison Fraker, Dean College of Environmental Design
UNIVERSITY OF CALIFORNIA, SAN DIEGO
Dr. Eduardo Macagno
Dr. Sonia Ancoli-Israel
THE NEW SCHOOL OF ARCHITECTURE & DESIGN
Terry Klein
Stephen LeSourd
RENSSELAER POLYTECHNIC INSTITUTE
Mariana Figuero, Ph.D.
NATIONAL INSTITUTES OF MENTAL HEALTH
Esther M. Sternberg, M.D.
SMITH GROUP
Duc Manh Tran (Chong/Smith Group)
DAYSIMETER
Dr. Mark Rae
Dr. Andrew Bierman
LIGHTBOOK,INC.
SILVERMAN AND LIGHT
Chuck Silverman
KAISER PERMANENTE
Thanks to the following individuals who gave of their time and expertise to make this project a success.
John Kouletsis, Director, Strategy, Planning, and Design
Dr. Joe Selby, Director, Northern California Division of Research
Christine Malcolm, Sr. Vice President, Hospital Strategy and National Facilities
Dr. Dave Newhouse, Associate Physician in Chief, Fremont Medical Center
Katie Holmes, Leader, Service Enhancement
Abelardo Ruiz, Sr. Project Manager, NFS Care Environment
Linda Raker, Sr. Project Manager, NFS Care Environment
Ronald Knox, Vice President, National Diversity
Gayle Tang, Director, National Linguistic and Cultural Programs, National Diversity
Marty Kaplan, PhD
Mike Mannina, National Manager, NFS CAFM Services
Michael Schroeder, Project Manager, NFS Care Environment
Wenbin Mo, PhD, Senior Data Consultant, National Market Research
Joan Wu, Data Consultant, National Market Research
Janet Ban, Senior Data Consultant, National Market Research
Long Ngo, PhD, Senior Data Consultant, National Market Research
Perry Class; Josh Lail; Loleatha Robertson; Joe Yun; Lan Nguyen; Harry Cho
[14] Grant recipient Chong Partners Architecture is now Stantec Architecture, University of California Berkeley, and Kaiser Permanente